Heart Failure Reviews ( IF 4.6 ) Pub Date : 2023-09-14 , DOI: 10.1007/s10741-023-10345-y Filippos Triposkiadis 1 , Alexandros Briasoulis 2 , Takeshi Kitai 3 , Dimitrios Magouliotis 4 , Thanos Athanasiou 5 , John Skoularigis 6 , Andrew Xanthopoulos 6
|
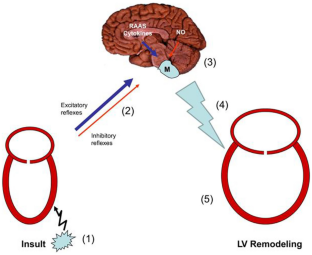
Several attempts have been made, by the scientific community, to develop a unifying hypothesis that explains the clinical syndrome of heart failure (HF). The currently widely accepted neurohormonal model has substituted the cardiorenal and the cardiocirculatory models, which focused on salt-water retention and low cardiac output/peripheral vasoconstriction, respectively. According to the neurohormonal model, HF with eccentric left ventricular (LV) hypertrophy (LVH) (systolic HF or HF with reduced LV ejection fraction [LVEF] or HFrEF) develops and progresses because endogenous neurohormonal systems, predominantly the sympathetic nervous system (SNS) and the renin–angiotensin–aldosterone system (RAAS), exhibit prolonged activation following the initial heart injury exerting deleterious hemodynamic and direct nonhemodynamic cardiovascular effects. However, there is evidence to suggest that SNS overactivity often preexists HF development due to its association with HF risk factors, is also present in HF with preserved LVEF (diastolic HF or HFpEF), and that it is linked to immune/inflammatory factors. Furthermore, SNS activity in HF may be augmented by coexisting noncardiac morbidities and modified by genetic factors and demographics. The purpose of this paper is to provide a contemporary overview of the complex associations between SNS overactivity and the development and progression of HF, summarize the underlying mechanisms, and discuss the clinical implications as they relate to therapeutic interventions mitigating SNS overactivity.
中文翻译:
重新审视心力衰竭中的交感神经系统
科学界已经进行了多次尝试,试图提出一个统一的假说来解释心力衰竭 (HF) 的临床综合征。目前广泛接受的神经激素模型已经取代了心肾模型和心循环模型,后者分别关注盐水潴留和低心输出量/外周血管收缩。根据神经激素模型,伴有偏心性左心室 (LV) 肥厚 (LVH) 的心力衰竭(收缩期心力衰竭或左心室射血分数降低的心力衰竭 [LVEF] 或 HFrEF)的发生和进展是因为内源性神经激素系统,主要是交感神经系统 (SNS)肾素-血管紧张素-醛固酮系统(RAAS)在最初的心脏损伤后表现出长时间的激活,产生有害的血流动力学和直接的非血流动力学心血管效应。然而,有证据表明,SNS 过度活跃通常先于心力衰竭发生,因为它与心力衰竭危险因素有关,也存在于 LVEF 保留的心力衰竭(舒张期心力衰竭或 HFpEF)中,并且与免疫/炎症因素有关。此外,心力衰竭中的 SNS 活性可能会因共存的非心脏疾病而增强,并会因遗传因素和人口统计学因素而改变。本文的目的是提供 SNS 过度活跃与心力衰竭发生和进展之间复杂关联的当代概述,总结潜在机制,并讨论与减轻 SNS 过度活跃的治疗干预相关的临床意义。


























 京公网安备 11010802027423号
京公网安备 11010802027423号