Heart and Vessels ( IF 1.5 ) Pub Date : 2023-12-16 , DOI: 10.1007/s00380-023-02343-9 Eitaro Kodani , Hiroshi Inoue , Hirotsugu Atarashi , Ken Okumura , Takeshi Yamashita , Hideki Origasa ,
|
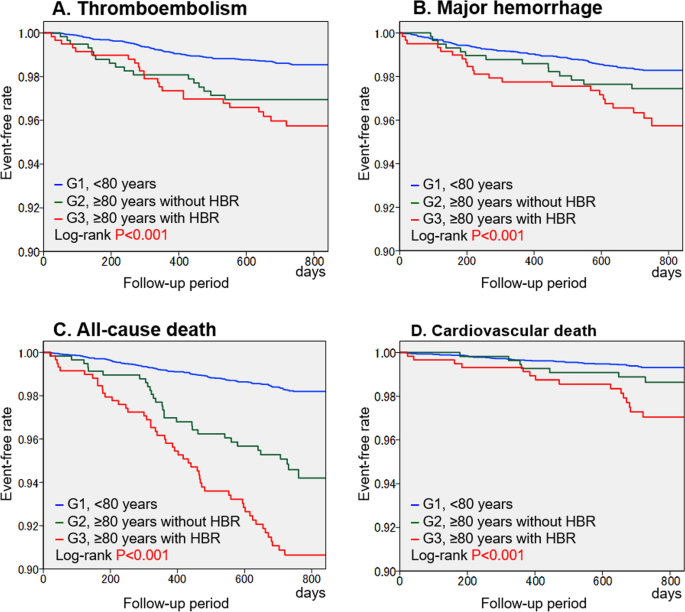
Recently, a once-daily dose of edoxaban (15-mg) has been approved for stroke prevention in non-valvular atrial fibrillation (NVAF) patients aged ≥ 80 years, in whom standard oral anticoagulants are not recommended because of high bleeding risk (HBR), based on the ELDERCARE-AF trial. However, information regarding the characteristics and clinical outcomes among such patients is limited. Thus, this study aimed to clarify the characteristics and event rates in elderly patients with NVAF and HBR defined by the ELDERCARE-AF criteria. Of the 7406 NVAF outpatients included in the J-RHYTHM Registry, 60 patients with creatinine clearance (CrCl) < 15 mL/min were excluded. The remaining 7346 patients (age, 69.7 ± 9.9 years; men, 70.9%; warfarin use, 78.7%) were divided into three groups: Group 1, aged < 80 years (n = 6165); Group 2, aged ≥ 80 years without HBR (n = 584); and Group 3, aged ≥ 80 years with HBR (at least one of the followings; CrCl, 15–30 mL/min, history of bleeding, body weight ≤ 45 kg, and antiplatelet use) (n = 597, eligible for 15-mg edoxaban). Patients in Group 3 had a higher prevalence of comorbidities, and therefore, both higher thromboembolic and bleeding risk scores than in the other groups. During the 2-year follow-up period, the incidence rates (per 100 person-years) of thromboembolism in Groups 1, 2, and 3 were 0.7, 1.5, and 2.1 (P < 0.001), major hemorrhage, 0.8, 1.2, and 2.0 (P < 0.001), and all-cause death, 0.8, 2.6, and 4.6 (P < 0.001), respectively. Adjusted hazard ratios of Group 3 were 1.64 (95% confidence interval 0.89–3.04, P = 0.116) for thromboembolism, 1.53 (0.85–2.72, P = 0.154) for major hemorrhage, and 1.84 (1.19–2.85, P = 0.006) for all-cause death compared with Group 1. The NVAF Patients aged ≥ 80 years with HBR defined by the ELDERCARE-AF criteria were certainly at a higher adverse event risk, especially for all-cause death. Clinical trial registration: The J-RHYTHM Registry is registered in the University Hospital Medicine Information Network (UMIN) Clinical Trials Registry (unique identifier: UMIN000001569) http://www.umin.ac.jp/ctr/.
中文翻译:
患有非瓣膜性心房颤动和高出血风险的老年患者的特征和结果:J-RHYTHM 注册表的亚分析
最近,每日一次剂量的艾多沙班(15 毫克)已被批准用于年龄 ≥ 80 岁的非瓣膜性心房颤动 (NVAF) 患者的卒中预防,由于出血风险高,不建议使用标准口服抗凝剂 (HBR) ),基于 ELDERCARE-AF 试验。然而,有关此类患者的特征和临床结果的信息有限。因此,本研究旨在阐明 ELDERCARE-AF 标准定义的 NVAF 和 HBR 老年患者的特征和事件发生率。在 J-RHYTHM 登记处纳入的 7406 名 NVAF 门诊患者中,排除了 60 名肌酐清除率 (CrCl) < 15 mL/min 的患者。其余 7346 名患者(年龄,69.7 ± 9.9 岁;男性,70.9%;使用华法林,78.7%)被分为三组:第 1 组,年龄 < 80 岁(n = 6165);第 1 组,年龄 < 80 岁(n = 6165);第 2 组,年龄 ≥ 80 岁,无 HBR (n = 584);第 3 组,年龄 ≥ 80 岁,患有 HBR(至少满足以下条件之一:CrCl,15-30 mL/min,出血史,体重 ≤ 45 kg,使用抗血小板药物)(n = 597,符合 15-毫克艾多沙班)。第 3 组患者的合并症患病率较高,因此血栓栓塞和出血风险评分均高于其他组。 2年随访期间,第1、2、3组血栓栓塞发生率(每100人年)分别为0.7、1.5、2.1(P < 0.001),大出血为0.8、1.2、和 2.0 (P < 0.001),全因死亡分别为 0.8、2.6 和 4.6 (P < 0.001)。第 3 组的血栓栓塞调整后风险比为 1.64(95% 置信区间 0.89-3.04,P = 0.116),大出血为 1.53(0.85-2.72,P = 0.154),大出血为 1.84(1.19-2.85,P = 0.006)。与第 1 组相比,全因死亡。 根据 ELDERCARE-AF 标准定义的年龄≥ 80 岁且患有 HBR 的 NVAF 患者无疑面临较高的不良事件风险,尤其是全因死亡。临床试验注册:J-RHYTHM 注册中心在大学医院医学信息网络 (UMIN) 临床试验注册中心注册(唯一标识符:UMIN000001569)http://www.umin.ac.jp/ctr/。


























 京公网安备 11010802027423号
京公网安备 11010802027423号