Journal of Human Hypertension ( IF 2.7 ) Pub Date : 2024-01-20 , DOI: 10.1038/s41371-023-00888-w Nadège Côté , Catherine Fortier , Louis-Charles Desbiens , János Nemcsik , Mohsen Agharazii
|
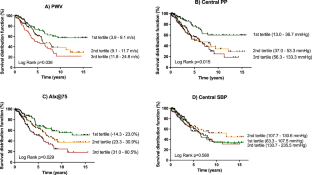
Aortic stiffness, measured by carotid-femoral pulse wave velocity (PWV), is a predictor of cardiovascular (CV) mortality in patients with end-stage renal disease (ESRD). Aortic stiffness increases aortic systolic and pulse pressures (cSBP, cPP) and augmentation index adjusted for a heart rate of 75 beats per minute (AIx@75). In this study, we examined if the integration of multiple components of central blood pressure and aortic stiffness (ICPS) into risk score categories could improve CV mortality prediction in ESRD. In a prospective cohort of 311 patients with ESRD on dialysis who underwent vascular assessment at baseline, 118 CV deaths occurred after a median follow-up of 3.1 years. The relationship between hemodynamic parameters and CV mortality was analyzed through Kaplan–Meier and Cox survival analysis. ICPS risk score from 0 to 5 points were calculated from points given to tertiles, and were regrouped into three risk categories (Average, High, Very-High). A strong association was found between the ICPS risk categories and CV mortality (High risk HR = 2.20, 95% CI: 1.05–4.62, P = 0.036); Very-High risk (HR = 4.44, 95% CI: 2.21–8.92, P < 0.001) as compared to the Average risk group. The Very-High risk category remained associated with CV mortality (HR = 3.55, 95% CI: 1.37–9.21, P = 0.009) after adjustment for traditional CV risk factors as compared to the Average risk group. While higher C-statistics value of ICPS categories (C: 0.627, 95% CI: 0.578–0.676, P = 0.001) was not statistically superior to PWV, cPP or AIx@75, the use of ICPS categories resulted in a continuous net reclassification index of 0.56 (95% CI: 0.07–0.99). In conclusion, integration of multiple components of central blood pressure and aortic stiffness may potentially be useful for better prediction of CV mortality in this cohort.
中文翻译:
个体与综合中心血压和主动脉僵硬度在预测终末期肾病心血管死亡率方面的比较
通过颈动脉-股动脉脉搏波速度 (PWV) 测量的主动脉僵硬度是终末期肾病 (ESRD) 患者心血管 (CV) 死亡率的预测因子。主动脉僵硬会增加主动脉收缩压和脉压(cSBP、cPP)以及根据每分钟 75 次心率调整的增强指数 (AIx@75)。在这项研究中,我们研究了将中心血压和主动脉僵硬度 (ICPS) 的多个组成部分整合到风险评分类别中是否可以改善 ESRD 的心血管死亡率预测。在一个由 311 名接受透析的 ESRD 患者组成的前瞻性队列中,他们在基线时接受了血管评估,中位随访 3.1 年后,有 118 名心血管死亡。通过 Kaplan-Meier 和 Cox 生存分析分析血流动力学参数与 CV 死亡率之间的关系。ICPS 风险评分从 0 到 5 分是根据三分位数的分数计算出来的,并重新分为三个风险类别(平均、高、非常高)。ICPS 风险类别与 CV 死亡率之间存在很强的相关性(高风险HR = 2.20,95% CI:1.05–4.62,P = 0.036); 与平均风险组相比,极高风险(HR = 4.44,95% CI:2.21–8.92,P < 0.001)。 与平均风险组相比,在调整传统心血管风险因素后,极高风险类别仍然与心血管死亡率相关(HR = 3.55,95% CI:1.37-9.21,P = 0.009)。虽然 ICPS 类别的较高 C 统计值(C:0.627,95% CI:0.578–0.676,P = 0.001)在统计上并不优于 PWV、cPP 或 AIx@75,但 ICPS 类别的使用导致了连续的净重新分类指数为 0.56(95% CI:0.07-0.99)。总之,中心血压和主动脉僵硬度的多个组成部分的整合可能有助于更好地预测该队列中的心血管死亡率。


























 京公网安备 11010802027423号
京公网安备 11010802027423号