当前位置:
X-MOL 学术
›
J. Cardiovasc. Comput. Tomogr.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
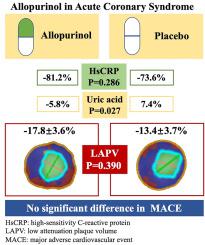
No evidence of coronary plaque stabilization by allopurinol in patients with acute coronary syndrome
Journal of Cardiovascular Computed Tomography ( IF 5.4 ) Pub Date : 2024-01-23 , DOI: 10.1016/j.jcct.2024.01.013 Miao Yu , Jin Gu , He-Shui Shi , Zheng-Feng Zhu , Fen Yang , Yuan-Fan Yuan , Xin-Xin Shuai , Yu-Miao Wei , Min Cheng , Jing Yuan , Tian Xie , Yong Yang , Da-Zhu Li , Min Zhang , Yong-Xin Lu , Ming Yang , You-Cai Zhou , Xiang Cheng
Journal of Cardiovascular Computed Tomography ( IF 5.4 ) Pub Date : 2024-01-23 , DOI: 10.1016/j.jcct.2024.01.013 Miao Yu , Jin Gu , He-Shui Shi , Zheng-Feng Zhu , Fen Yang , Yuan-Fan Yuan , Xin-Xin Shuai , Yu-Miao Wei , Min Cheng , Jing Yuan , Tian Xie , Yong Yang , Da-Zhu Li , Min Zhang , Yong-Xin Lu , Ming Yang , You-Cai Zhou , Xiang Cheng
|
Allopurinol, a xanthine inhibitor that lowers uric acid concentration, has been proven to reduce inflammation and oxidative stress in patients with cardiovascular disease. However, it is unknown whether these beneficial effects translate into favorable plaque modification in acute coronary syndromes (ACS). This study aimed to investigate whether allopurinol could improve coronary plaque stabilization using coronary computed tomography angiography (CCTA). This was a prospective, single-center, randomized, double-blind clinical trial began in March 2019. A total of 162 ACS patients aged 18–80 years with a blood level of high-sensitivity C-reactive protein (hsCRP) > 2 mg/L were included. The subjects were randomly assigned in a 1:1 ratio to receive either allopurinol sustained-release capsules (at a dose of 0.25 g once daily) or placebo for 12 months. The plaque analysis was performed at CCTA. The primary efficacy endpoint was the change in low-attenuation plaque volume (LAPV) from baseline to the 12-month follow-up. Among 162 patients, 54 in allopurinol group and 51 in placebo group completed the study. The median follow-up duration was 14 months in both groups. Compared with placebo, allopurinol therapy did not significantly alter LAPV (−13.4 ± 3.7 % vs. −17.8 ± 3.6 %, = 0.390), intermediate attenuation plaque volume (−16.1 ± 3.0 % vs. −16.2 ± 2.9 %, = 0.992), dense calcified plaque volume (12.2 ± 13.7 % vs. 9.7 ± 13.0 %, = 0.894), total atheroma volume (−15.2 ± 3.2 % vs. −16.4 ± 3.1 %, = 0.785), remodeling index (2.0 ± 3.9 % vs. 5.4 ± 3.8 %, = 0.536) or hsCRP levels (−73.6 [−91.6–17.9] % vs. −81.2 [−95.4–47.7] %, = 0.286). Our findings suggest that allopurinol does not improve atherosclerotic plaque stability or inflammation in ACS.
中文翻译:

没有证据表明别嘌呤醇可以稳定急性冠状动脉综合征患者的冠状动脉斑块
别嘌呤醇是一种降低尿酸浓度的黄嘌呤抑制剂,已被证明可以减少心血管疾病患者的炎症和氧化应激。然而,目前尚不清楚这些有益作用是否会转化为急性冠状动脉综合征(ACS)中有利的斑块改变。本研究旨在利用冠状动脉计算机断层扫描血管造影(CCTA)研究别嘌呤醇是否可以改善冠状动脉斑块稳定性。这是一项于 2019 年 3 月开始的前瞻性、单中心、随机、双盲临床试验。共有 162 名 18-80 岁的 ACS 患者,其血液中高敏 C 反应蛋白 (hsCRP) 水平>包括 2 毫克/升。受试者以 1:1 的比例随机分配接受别嘌呤醇缓释胶囊(剂量为 0.25 克,每日一次)或安慰剂,为期 12 个月。噬菌斑分析在 CCTA 进行。主要疗效终点是低衰减斑块体积 (LAPV) 从基线到 12 个月随访的变化。在 162 名患者中,别嘌呤醇组 54 名患者和安慰剂组 51 名患者完成了研究。两组的中位随访时间均为 14 个月。与安慰剂相比,别嘌呤醇治疗没有显着改变 LAPV(−13.4 ± 3.7 % vs. −17.8 ± 3.6 %,= 0.390)、中间衰减斑块体积(−16.1 ± 3.0 %)对比 -16.2 ± 2.9 %,= 0.992),致密钙化斑块体积(12.2 ± 13.7 % 对比 9.7± 13.0 %,= 0.894),总粥样斑块体积(− 15.2± 3.2 % 对比 -16.4 ± 3.1 %,= 0.785),重塑指数(2.0 ± 3.9 % 对比 5.4 ± 3.8 %,= 0.536)或hsCRP 水平(−73.6 [−91.6–17.9] % vs. −81.2 [−95.4–47.7] %,= 0.286)。我们的研究结果表明别嘌呤醇不能改善 ACS 中的动脉粥样硬化斑块稳定性或炎症。
更新日期:2024-01-23
中文翻译:
没有证据表明别嘌呤醇可以稳定急性冠状动脉综合征患者的冠状动脉斑块
别嘌呤醇是一种降低尿酸浓度的黄嘌呤抑制剂,已被证明可以减少心血管疾病患者的炎症和氧化应激。然而,目前尚不清楚这些有益作用是否会转化为急性冠状动脉综合征(ACS)中有利的斑块改变。本研究旨在利用冠状动脉计算机断层扫描血管造影(CCTA)研究别嘌呤醇是否可以改善冠状动脉斑块稳定性。这是一项于 2019 年 3 月开始的前瞻性、单中心、随机、双盲临床试验。共有 162 名 18-80 岁的 ACS 患者,其血液中高敏 C 反应蛋白 (hsCRP) 水平>包括 2 毫克/升。受试者以 1:1 的比例随机分配接受别嘌呤醇缓释胶囊(剂量为 0.25 克,每日一次)或安慰剂,为期 12 个月。噬菌斑分析在 CCTA 进行。主要疗效终点是低衰减斑块体积 (LAPV) 从基线到 12 个月随访的变化。在 162 名患者中,别嘌呤醇组 54 名患者和安慰剂组 51 名患者完成了研究。两组的中位随访时间均为 14 个月。与安慰剂相比,别嘌呤醇治疗没有显着改变 LAPV(−13.4 ± 3.7 % vs. −17.8 ± 3.6 %,= 0.390)、中间衰减斑块体积(−16.1 ± 3.0 %)对比 -16.2 ± 2.9 %,= 0.992),致密钙化斑块体积(12.2 ± 13.7 % 对比 9.7± 13.0 %,= 0.894),总粥样斑块体积(− 15.2± 3.2 % 对比 -16.4 ± 3.1 %,= 0.785),重塑指数(2.0 ± 3.9 % 对比 5.4 ± 3.8 %,= 0.536)或hsCRP 水平(−73.6 [−91.6–17.9] % vs. −81.2 [−95.4–47.7] %,= 0.286)。我们的研究结果表明别嘌呤醇不能改善 ACS 中的动脉粥样硬化斑块稳定性或炎症。


























 京公网安备 11010802027423号
京公网安备 11010802027423号