Journal of Human Hypertension ( IF 2.7 ) Pub Date : 2024-02-01 , DOI: 10.1038/s41371-024-00897-3 Willington Amutuhaire , Fred Collins Semitala , Isaac Derick Kimera , Christabellah Namugenyi , Frank Mulindwa , Rebecca Ssenyonjo , Rodgers Katwesigye , Frank Mugabe , Gerald Mutungi , Isaac Ssinabulya , Jeremy I. Schwartz , Anne R. Katahoire , Lewis S. Musoke , George A. Yendewa , Chris T. Longenecker , Martin Muddu
|
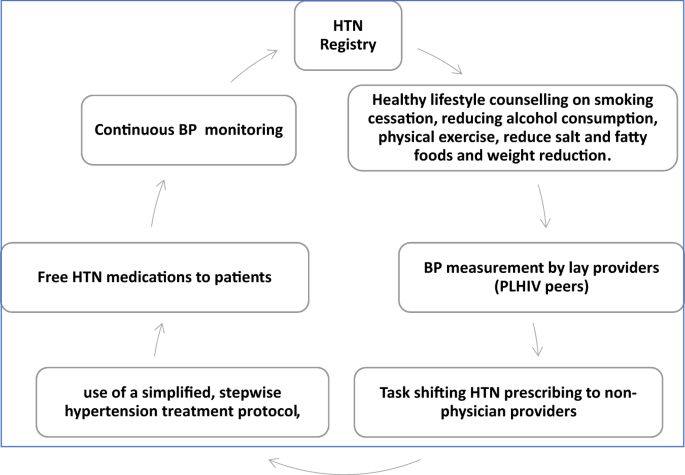
In this cohort study, we determined time to blood pressure (BP) control and its predictors among hypertensive PLHIV enrolled in integrated hypertension-HIV care based on the World Health Organization (WHO) HEARTS strategy at Mulago Immunosuppression Clinic in Uganda. From August 2019 to March 2020, we enrolled hypertensive PLHIV aged \(\ge\)18 years and initiated Amlodipine 5 mg mono-therapy for BP (140–159)/(90–99) mmHg or Amlodipine 5 mg/Valsartan 80 mg duo-therapy for BP ≥ 160/90 mmHg. Patients were followed with a treatment escalation plan until BP control, defined as BP < 140/90 mmHg. We used Cox proportional hazards models to identify predictors of time to BP control. Of 877 PLHIV enrolled (mean age 50.4 years, 62.1% female), 30% received mono-therapy and 70% received duo-therapy. In the monotherapy group, 66%, 88% and 96% attained BP control in the first, second and third months, respectively. For patients on duo-therapy, 56%, 83%, 88% and 90% achieved BP control in the first, second, third, and fourth months, respectively. In adjusted Cox proportional hazard analysis, higher systolic BP (aHR 0.995, 95% CI 0.989-0.999) and baseline ART tenofovir/lamivudine/efavirenz (aHR 0.764, 95% CI 0.637–0.917) were associated with longer time to BP control, while being on ART for >10 years was associated with a shorter time to BP control (aHR 1.456, 95% CI 1.126–1.883). The WHO HEARTS strategy was effective at achieving timely BP control among PLHIV. Additionally, monotherapy anti-hypertensive treatment for stage I hypertension is a viable option to achieve BP control and limit pill burden in resource limited HIV care settings.
中文翻译:
根据乌干达大型城市艾滋病毒诊所采用的 WHO HEARTS 实施策略,接受高血压和艾滋病毒综合治疗的患者的血压控制时间和预测因素
在这项队列研究中,我们根据乌干达穆拉戈免疫抑制诊所的世界卫生组织 (WHO) HEARTS 策略,确定了参加高血压 - HIV 综合护理的高血压 PLHIV 的血压 (BP) 控制时间及其预测因素。2019年8月至2020年3月,我们入组了18岁的高血压艾滋病毒感染者,并开始氨氯地平5 mg单药治疗血压(140-159)/(90-99)mmHg或氨氯地平5 mg/缬沙坦80 mg血压≥ 160/90 mmHg 的双重疗法。按照治疗升级计划对患者进行随访,直至血压控制(定义为血压<140/90 mmHg)。我们使用 Cox 比例风险模型来确定血压控制时间的预测因素。在 877 名登记的艾滋病毒感染者中(平均年龄 50.4 岁,62.1% 为女性),30% 接受单一治疗,70% 接受双重治疗。在单一疗法组中,分别有 66%、88% 和 96% 在第一个月、第二个月和第三个月达到血压控制。对于接受双联治疗的患者,分别有 56%、83%、88% 和 90% 在第一、第二、第三和第四个月实现血压控制。在调整后的 Cox 比例风险分析中,较高的收缩压(aHR 0.995,95% CI 0.989-0.999)和基线 ART 替诺福韦/拉米夫定/依非韦伦(aHR 0.764,95% CI 0.637-0.917)与较长的血压控制时间相关,而接受 ART 超过 10 年与血压控制时间较短相关(aHR 1.456,95% CI 1.126–1.883)。世卫组织心脏战略在及时控制艾滋病病毒感染者的血压方面是有效的。此外,在资源有限的艾滋病毒护理环境中,针对 I 期高血压的单一疗法抗高血压治疗是实现血压控制和限制药物负担的可行选择。


























 京公网安备 11010802027423号
京公网安备 11010802027423号