当前位置:
X-MOL 学术
›
J. Vasc. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Relevance of BEST-CLI trial endpoints in a tertiary care limb preservation program
Journal of Vascular Surgery ( IF 4.3 ) Pub Date : 2024-02-23 , DOI: 10.1016/j.jvs.2024.02.022 Iris H. Liu , Rym El Khoury , Jade S. Hiramoto , Warren J. Gasper , Peter A. Schneider , Shant M. Vartanian , Michael S. Conte
Journal of Vascular Surgery ( IF 4.3 ) Pub Date : 2024-02-23 , DOI: 10.1016/j.jvs.2024.02.022 Iris H. Liu , Rym El Khoury , Jade S. Hiramoto , Warren J. Gasper , Peter A. Schneider , Shant M. Vartanian , Michael S. Conte
|
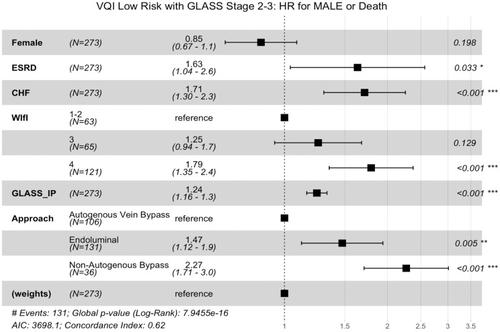
Major adverse limb event-free survival (MALE-FS) differed significantly by initial revascularization approach in the BEST-CLI randomized trial. The BEST-CLI trial represented a highly selected subgroup of patients seen in clinical practice; thus, we examined the endpoint of MALE-FS in an all-comers tertiary care practice setting. This is a single-center retrospective study of consecutive, unique patients who underwent technically successful infrainguinal revascularization for chronic limb-threatening ischemia (2011-2021). MALE was major amputation (transtibial or above) or major reintervention (new bypass, open bypass revision, thrombectomy, or thrombolysis). Among 469 subjects, the mean age was 70 years, and 34% were female. Characteristics included diabetes (68%), end-stage renal disease (ESRD) (16%), Wound, Ischemia, and foot Infection (WIfI) stage 4 (44%), Global Limb Anatomic Staging System (GLASS) stage 3 (62%), and high pedal artery calcium score (pMAC) (22%). Index revascularization was autogenous vein bypass (AVB) (30%), non-autogenous bypass (NAB) (13%), or endovascular (ENDO) (57%). The composite endpoint of MALE or death occurred in 237 patients (51%) at a median time of 189 days from index revascularization. In an adjusted Cox model, factors independently associated with MALE or death included younger age, ESRD, WIfI stage 4, higher GLASS stage, and moderate-severe pMAC, whereas AVB was associated with improved MALE-FS. Freedom from MALE-FS, MALE, and major amputation at 30 days were 90%, 92%, and 95%; and at 1 year were 63%, 70%, and 83%, respectively. MALE occurred in 144 patients (31%) and was associated with ESRD, WIfI stage, GLASS stage, pMAC score, and index revascularization approach. AVB had superior durability, with adjusted 2-year freedom from MALE of 72%, compared with 66% for ENDO and 51% for NAB. Within the AVB group, spliced vein conduit had higher MALE compared with single-segment vein (hazard ratio, 1.8; 95% confidence interval, 0.9-3.7; = .008 after inverse propensity weighting), but there was no statistically significant difference in major amputation. Of the 144 patients with any MALE, the first MALE was major reintervention in 47% and major amputation in 53%. Major amputation as first MALE was associated with non-AVB index approach. Indications for major reintervention were symptomatic stenosis/occlusion (54%), lack of clinical improvement (28%), asymptomatic graft stenosis (16%), and iatrogenic events (3%). Conversion to bypass occurred after 6% of ENDO cases, two-thirds of which involved distal bypass targets at the ankle or foot. In this consecutive, all-comers cohort, disease complexity was associated with procedural selection and MALE-FS. AVB independently provided the greatest MALE-FS and freedom from MALE and major amputation. Compared with the BEST-CLI randomized trial, MALE after ENDO in this series was more frequently major amputation, with relatively few conversions to open bypass.
中文翻译:

BEST-CLI 试验终点在三级护理肢体保存计划中的相关性
在 BEST-CLI 随机试验中,初始血运重建方法的主要不良肢体无事件生存期 (MALE-FS) 存在显着差异。 BEST-CLI 试验代表了临床实践中经过精心挑选的患者亚组;因此,我们在所有参与者的三级护理实践环境中检查了 MALE-FS 的终点。这是一项单中心回顾性研究,研究对象为连续、独特的患者,这些患者在 2011-2021 年期间因慢性肢体威胁性缺血而接受了技术上成功的腹股沟下血运重建术。 MALE 是主要截肢(经胫骨或以上)或主要再干预(新搭桥、开放式搭桥翻修、血栓切除术或溶栓)。 469 名受试者中,平均年龄为 70 岁,其中 34% 为女性。特征包括糖尿病 (68%)、终末期肾病 (ESRD) (16%)、伤口、缺血和足部感染 (WIfI) 第 4 期 (44%)、全球肢体解剖分期系统 (GLASS) 第 3 期 (62 %) 和高足动脉钙化评分 (pMAC) (22%)。血运重建指标为自体静脉搭桥术 (AVB) (30%)、非自体静脉搭桥术 (NAB) (13%) 或血管内搭桥术 (ENDO) (57%)。 237 名患者(51%)在指数血运重建后的中位时间 189 天发生了 MALE 或死亡的复合终点。在调整后的 Cox 模型中,与 MALE 或死亡独立相关的因素包括年龄较小、ESRD、WIfI 4 期、较高的 GLASS 分期和中重度 pMAC,而 AVB 与 MALE-FS 改善相关。 30 天时免于 MALE-FS、MALE 和大截肢的比例分别为 90%、92% 和 95%; 1 年时的比率分别为 63%、70% 和 83%。 144 名患者 (31%) 发生 MALE,且与 ESRD、WIfI 分期、GLASS 分期、pMAC 评分和指数血运重建方法相关。 AVB 具有卓越的耐用性,调整后的 2 年无 MALE 率为 72%,而 ENDO 为 66%,NAB 为 51%。在 AVB 组中,与单段静脉相比,拼接静脉导管具有更高的 MALE(风险比,1.8;95% 置信区间,0.9-3.7;逆倾向加权后 = 0.008),但主要差异无统计学意义。截肢。在 144 名患有任何 MALE 的患者中,首次 MALE 患者中 47% 进行了重大再干预,53% 进行了重大截肢。第一次 MALE 的大截肢与非 AVB 索引方法相关。主要再干预的指征是有症状的狭窄/闭塞(54%)、缺乏临床改善(28%)、无症状的移植物狭窄(16%)和医源性事件(3%)。 6% 的 ENDO 病例发生转为旁路手术,其中三分之二涉及踝关节或足部的远端旁路手术目标。在这个连续的、所有参与者的队列中,疾病复杂性与程序选择和 MALE-FS 相关。 AVB 独立提供了最大的 MALE-FS 并免于 MALE 和大截肢。与BEST-CLI随机试验相比,该系列中ENDO后的MALE更频繁地发生大截肢,转为开放搭桥的情况相对较少。
更新日期:2024-02-23
中文翻译:
BEST-CLI 试验终点在三级护理肢体保存计划中的相关性
在 BEST-CLI 随机试验中,初始血运重建方法的主要不良肢体无事件生存期 (MALE-FS) 存在显着差异。 BEST-CLI 试验代表了临床实践中经过精心挑选的患者亚组;因此,我们在所有参与者的三级护理实践环境中检查了 MALE-FS 的终点。这是一项单中心回顾性研究,研究对象为连续、独特的患者,这些患者在 2011-2021 年期间因慢性肢体威胁性缺血而接受了技术上成功的腹股沟下血运重建术。 MALE 是主要截肢(经胫骨或以上)或主要再干预(新搭桥、开放式搭桥翻修、血栓切除术或溶栓)。 469 名受试者中,平均年龄为 70 岁,其中 34% 为女性。特征包括糖尿病 (68%)、终末期肾病 (ESRD) (16%)、伤口、缺血和足部感染 (WIfI) 第 4 期 (44%)、全球肢体解剖分期系统 (GLASS) 第 3 期 (62 %) 和高足动脉钙化评分 (pMAC) (22%)。血运重建指标为自体静脉搭桥术 (AVB) (30%)、非自体静脉搭桥术 (NAB) (13%) 或血管内搭桥术 (ENDO) (57%)。 237 名患者(51%)在指数血运重建后的中位时间 189 天发生了 MALE 或死亡的复合终点。在调整后的 Cox 模型中,与 MALE 或死亡独立相关的因素包括年龄较小、ESRD、WIfI 4 期、较高的 GLASS 分期和中重度 pMAC,而 AVB 与 MALE-FS 改善相关。 30 天时免于 MALE-FS、MALE 和大截肢的比例分别为 90%、92% 和 95%; 1 年时的比率分别为 63%、70% 和 83%。 144 名患者 (31%) 发生 MALE,且与 ESRD、WIfI 分期、GLASS 分期、pMAC 评分和指数血运重建方法相关。 AVB 具有卓越的耐用性,调整后的 2 年无 MALE 率为 72%,而 ENDO 为 66%,NAB 为 51%。在 AVB 组中,与单段静脉相比,拼接静脉导管具有更高的 MALE(风险比,1.8;95% 置信区间,0.9-3.7;逆倾向加权后 = 0.008),但主要差异无统计学意义。截肢。在 144 名患有任何 MALE 的患者中,首次 MALE 患者中 47% 进行了重大再干预,53% 进行了重大截肢。第一次 MALE 的大截肢与非 AVB 索引方法相关。主要再干预的指征是有症状的狭窄/闭塞(54%)、缺乏临床改善(28%)、无症状的移植物狭窄(16%)和医源性事件(3%)。 6% 的 ENDO 病例发生转为旁路手术,其中三分之二涉及踝关节或足部的远端旁路手术目标。在这个连续的、所有参与者的队列中,疾病复杂性与程序选择和 MALE-FS 相关。 AVB 独立提供了最大的 MALE-FS 并免于 MALE 和大截肢。与BEST-CLI随机试验相比,该系列中ENDO后的MALE更频繁地发生大截肢,转为开放搭桥的情况相对较少。


























 京公网安备 11010802027423号
京公网安备 11010802027423号