当前位置:
X-MOL 学术
›
Clin. Gastroenterol. Hepatol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Outcomes of High-Grade Immune Checkpoint Inhibitor Hepatitis in Hospitalized and Nonhospitalized Patients
Clinical Gastroenterology and Hepatology ( IF 12.6 ) Pub Date : 2024-02-23 , DOI: 10.1016/j.cgh.2024.02.006 Michael Li , Danny Wong , Jordan S. Sack , Alexander S. Vogel , F. Stephen Hodi , Lawrence Fong , Jennifer C. Lai , Stephen D. Zucker , Shilpa Grover
Clinical Gastroenterology and Hepatology ( IF 12.6 ) Pub Date : 2024-02-23 , DOI: 10.1016/j.cgh.2024.02.006 Michael Li , Danny Wong , Jordan S. Sack , Alexander S. Vogel , F. Stephen Hodi , Lawrence Fong , Jennifer C. Lai , Stephen D. Zucker , Shilpa Grover
|
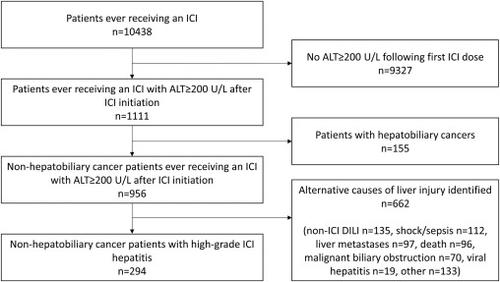
Guidelines recommend hospitalization for severe immune checkpoint inhibitor (ICI) hepatitis. We compared patient outcomes in the inpatient versus outpatient settings. We conducted a multicenter, retrospective cohort study of 294 ICI-treated patients who developed grade 3-4 ICI hepatitis. The primary outcome was time to alanine aminotransferase (ALT) normalization (≤40); secondary outcomes included time to ALT ≤100 U/L and time to death. To account for confounding by indication, inverse probability of treatment weighting was applied to perform Cox regression. A sensitivity analysis was performed excluding patients with grade 4 hepatitis. One hundred and sixty-six patients (56.5%) were hospitalized for a median of 6 (interquartile range, 3–11) days. On inverse probability of treatment weighting Cox regression, hospitalization was not associated with time to ALT normalization (hazard ratio [HR], 1.11; 95% confidence interval [CI], 0.86–1.43; = .436) or time to ALT ≤100 U/L (HR, 1.11; 95% CI, 0.86–1.43; = .420). In the sensitivity analysis limited to patients with grade 3 hepatitis, hospitalization was also not associated with time to ALT normalization (HR, 1.11; 95% CI, 0.83–1.50; = .474) or time to ALT ≤100 U/L (HR, 1.19; 95% CI, 0.90–1.58; = .225). In a subgroup analysis of 152 patients with melanoma, hospitalization was not associated with reduced risk of all-cause death (HR, 0.93; 95% CI, 0.53–1.64; = .798). Notably, despite their Common Terminology Criteria for Adverse Events classification of high-grade hepatitis, 94% of patients had “mild” liver injury based on International Drug-Induced Liver Injury Criteria. Hospitalization of patients with high-grade ICI hepatitis was not associated with faster hepatitis resolution and did not affect mortality. Routine hospitalization may not be necessary in all patients with high-grade ICI hepatitis and Common Terminology Criteria for Adverse Events criteria may overestimate severity of liver injury.
中文翻译:

住院和非住院患者的高级免疫检查点抑制剂肝炎的结果
指南建议因严重免疫检查点抑制剂(ICI)肝炎而住院。我们比较了住院患者和门诊患者的治疗结果。我们对 294 名接受 ICI 治疗且出现 3-4 级 ICI 肝炎的患者进行了一项多中心、回顾性队列研究。主要结局是丙氨酸氨基转移酶(ALT)正常化的时间(≤40);次要结局包括 ALT ≤ 100 U/L 的时间和死亡时间。为了解释适应症的混杂因素,应用治疗加权的逆概率来执行 Cox 回归。进行敏感性分析,排除 4 级肝炎患者。 166 名患者 (56.5%) 住院时间中位数为 6 天(四分位距,3-11)天。根据治疗加权 Cox 回归的逆概率,住院与 ALT 正常化时间(风险比 [HR],1.11;95% 置信区间 [CI],0.86–1.43;= .436)或 ALT ≤ 100 U 时间无关/L(HR,1.11;95% CI,0.86–1.43;= .420)。在仅限于 3 级肝炎患者的敏感性分析中,住院治疗也与 ALT 正常化时间 (HR, 1.11; 95% CI, 0.83–1.50; = .474) 或 ALT ≤ 100 U/L 时间 (HR, 1.11; ,1.19;95% CI,0.90–1.58;= .225)。在对 152 名黑色素瘤患者进行的亚组分析中,住院治疗与全因死亡风险降低无关(HR,0.93;95% CI,0.53–1.64;= .798)。值得注意的是,尽管其不良事件通用术语标准对高度肝炎进行了分类,但根据国际药物性肝损伤标准,94% 的患者出现“轻度”肝损伤。重度 ICI 肝炎患者的住院治疗与肝炎消退速度加快无关,也不影响死亡率。并非所有重度 ICI 肝炎患者都需要常规住院治疗,不良事件通用术语标准可能会高估肝损伤的严重程度。
更新日期:2024-02-23
中文翻译:
住院和非住院患者的高级免疫检查点抑制剂肝炎的结果
指南建议因严重免疫检查点抑制剂(ICI)肝炎而住院。我们比较了住院患者和门诊患者的治疗结果。我们对 294 名接受 ICI 治疗且出现 3-4 级 ICI 肝炎的患者进行了一项多中心、回顾性队列研究。主要结局是丙氨酸氨基转移酶(ALT)正常化的时间(≤40);次要结局包括 ALT ≤ 100 U/L 的时间和死亡时间。为了解释适应症的混杂因素,应用治疗加权的逆概率来执行 Cox 回归。进行敏感性分析,排除 4 级肝炎患者。 166 名患者 (56.5%) 住院时间中位数为 6 天(四分位距,3-11)天。根据治疗加权 Cox 回归的逆概率,住院与 ALT 正常化时间(风险比 [HR],1.11;95% 置信区间 [CI],0.86–1.43;= .436)或 ALT ≤ 100 U 时间无关/L(HR,1.11;95% CI,0.86–1.43;= .420)。在仅限于 3 级肝炎患者的敏感性分析中,住院治疗也与 ALT 正常化时间 (HR, 1.11; 95% CI, 0.83–1.50; = .474) 或 ALT ≤ 100 U/L 时间 (HR, 1.11; ,1.19;95% CI,0.90–1.58;= .225)。在对 152 名黑色素瘤患者进行的亚组分析中,住院治疗与全因死亡风险降低无关(HR,0.93;95% CI,0.53–1.64;= .798)。值得注意的是,尽管其不良事件通用术语标准对高度肝炎进行了分类,但根据国际药物性肝损伤标准,94% 的患者出现“轻度”肝损伤。重度 ICI 肝炎患者的住院治疗与肝炎消退速度加快无关,也不影响死亡率。并非所有重度 ICI 肝炎患者都需要常规住院治疗,不良事件通用术语标准可能会高估肝损伤的严重程度。


























 京公网安备 11010802027423号
京公网安备 11010802027423号