Cancer Immunology, Immunotherapy ( IF 5.8 ) Pub Date : 2024-03-02 , DOI: 10.1007/s00262-024-03643-3 Tanguy Y. Seiwert , Sophie Wildsmith , Jérôme Fayette , Kevin Harrington , Maura Gillison , Myung-Ju Ahn , Shunji Takahashi , Jared Weiss , Jean-Pascal Machiels , Shrujal Baxi , Valerie Baker , Brent Evans , Nassim Morsli , Jill Walker , Katia Real , Anne L’Hernault , Amanda Psyrri
|
Background
Selective biomarkers may improve outcomes in patients with recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC) treated with immune checkpoint inhibitor therapy. We investigated three independent biomarkers for association with efficacy in the randomized, phase III KESTREL study (NCT02551159) of first-line durvalumab monotherapy or durvalumab plus tremelimumab versus the EXTREME regimen: programmed cell death ligand-1 (PD-L1) immunohistochemistry, blood tumor mutational burden (bTMB) via circulating tumor DNA, and neutrophil-to-lymphocyte ratio (NLR).
Methods
Tumor or blood samples from patients enrolled in the KESTREL study were analyzed for PD-L1, bTMB, and NLR. Associations with overall survival (OS) or objective response rates (ORRs) were evaluated based on prespecified cut-offs for PD-L1 (tumor cell [TC] ≥ 50%/immune cell ≥ 25% or TC ≥ 25%), bTMB (≥ 16 mutations [mut] per megabase [Mb]), and NLR (≤ 7). Ad hoc analyses of exploratory cut-offs were performed.
Results
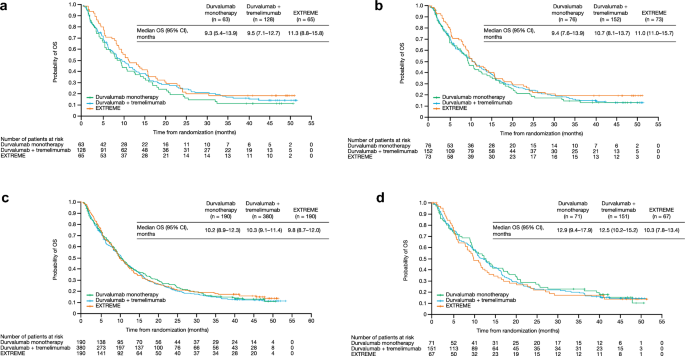
Prespecified or exploratory cut-offs for PD-L1 did not enrich for ORR or OS for durvalumab monotherapy or durvalumab plus tremelimumab versus EXTREME. In the bTMB ≥ 16 mut/Mb subgroup, OS hazard ratios (95% confidence interval) for durvalumab monotherapy and durvalumab plus tremelimumab versus EXTREME were 0.90 (0.48–1.72) and 0.69 (0.39–1.25), respectively. Complete response rates were 8.6% with durvalumab plus tremelimumab and 4.3% with EXTREME (≥ 16 mut/Mb subgroup). No improvement in OS was observed for durvalumab monotherapy or durvalumab plus tremelimumab versus EXTREME at prespecified or exploratory NLR cut-offs.
Conclusions
bTMB demonstrated potential utility for selecting patients with R/M HNSCC who benefited from durvalumab with or without tremelimumab versus EXTREME.
Trial registration ClinicalTrials.gov identifier NCT02551159.
中文翻译:
KESTREL 研究中 durvalumab 和 tremelimumab 在复发性或转移性头颈鳞状细胞癌中的生物标志物选择亚组的结果
背景
选择性生物标志物可以改善接受免疫检查点抑制剂治疗的复发性或转移性头颈鳞状细胞癌 (R/M HNSCC) 患者的预后。我们在一线 durvalumab 单药治疗或 durvalumab 加 tremelimumab 与 EXTREME 方案的随机 III 期 KESTREL 研究 (NCT02551159) 中研究了与疗效相关的三个独立生物标志物:程序性细胞死亡配体-1 (PD-L1) 免疫组织化学、血液肿瘤通过循环肿瘤 DNA 和中性粒细胞与淋巴细胞比率 (NLR) 检测突变负荷 (bTMB)。
方法
对参加 KESTREL 研究的患者的肿瘤或血液样本进行 PD-L1、bTMB 和 NLR 分析。根据预先设定的 PD-L1 临界值(肿瘤细胞 [TC] ≥ 50%/免疫细胞 ≥ 25% 或 TC ≥ 25%)、bTMB(每兆碱基 [Mb] ≥ 16 个突变 [mut]),且 NLR (≤ 7)。对探索性截止点进行了特别分析。
结果
与 EXTREME 相比,预先设定的或探索性的 PD-L1 临界点并没有丰富 durvalumab 单药治疗或 durvalumab 加 tremelimumab 的 ORR 或 OS。在 bTMB ≥ 16 mut/Mb 亚组中,durvalumab 单药治疗和 durvalumab 加 tremelimumab 与 EXTREME 相比,OS 风险比(95% 置信区间)分别为 0.90 (0.48–1.72) 和 0.69 (0.39–1.25)。durvalumab 加 tremelimumab 的完全缓解率为 8.6%,EXTREME(≥ 16 mut/Mb 亚组)的完全缓解率为 4.3%。在预先指定或探索性 NLR 截止值下,与 EXTREME 相比,durvalumab 单药治疗或 durvalumab 加 tremelimumab 未观察到 OS 改善。
结论
与 EXTREME 相比,bTMB 对于选择从 durvalumab 联合或不联合 tremelimumab 获益的 R/M HNSCC 患者具有潜在的实用性。
试验注册ClinicalTrials.gov 标识符 NCT02551159。


























 京公网安备 11010802027423号
京公网安备 11010802027423号