当前位置:
X-MOL 学术
›
Mayo Clin. Proc.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Emulated Trial for Discharge Prescription of Guideline-Directed Medical Therapy and 15-Year Survival After Coronary Artery Bypass Graft Surgery
Mayo Clinic Proceedings ( IF 8.9 ) Pub Date : 2024-03-07 , DOI: 10.1016/j.mayocp.2023.06.022 Yaron Moshkovitz , Liat Orenstein , Liraz Olmer , Keren Laufer , Arnona Ziv , Rachel Dankner
Mayo Clinic Proceedings ( IF 8.9 ) Pub Date : 2024-03-07 , DOI: 10.1016/j.mayocp.2023.06.022 Yaron Moshkovitz , Liat Orenstein , Liraz Olmer , Keren Laufer , Arnona Ziv , Rachel Dankner
|
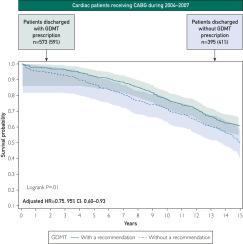
To explore admission and discharge prescription rates of guideline-directed medical therapy (GDMT), defined as aggregate antiplatelet agents, statins, and β-blockers, after coronary artery bypass graft (CABG) surgery and to reveal its association with long-term survival. This is a prospective cohort study–based emulated trial of patients undergoing elective or semi-elective isolated CABG surgery in 7 cardiothoracic units in Israel from January 1, 2004, to December 31, 2007, and followed up until December 31, 2020, for all-cause mortality. Only 59.2% of 968 patients (n=573) were discharged on GDMT after CABG surgery. Admission GDMT use conferred a 7 times greater likelihood of discharge GDMT prescription (odds ratio, 7.07; 95% CI, 5.04 to 9.91; <.001), with no sex differences observed. After applying inverse probability of treatment weighting, baseline characteristics were well balanced between groups. During a median follow-up of 13.7 years, a Cox regression model with propensity score–adjusted inverse probability of treatment weighting revealed lower mortality in patients with discharge GDMT prescription who underwent CABG surgery than in their counterparts (hazard ratio, 0.75; 95% CI, 0.60 to 0.93; =.008). The use of aggregate GDMT before surgery conferred a greater likelihood of GDMT prescription upon discharge, which, in turn, is associated with better long-term survival. Educational efforts of pertinent medical professionals are needed to minimize preventive treatment gaps. clinicaltrials.gov Identifier: NCT00356863
中文翻译:

指南指导药物治疗的出院处方与冠状动脉搭桥手术后 15 年生存率的模拟试验
探讨冠状动脉搭桥术 (CABG) 术后指南指导药物治疗 (GDMT)(定义为聚合抗血小板药物、他汀类药物和 β 受体阻滞剂)的入院和出院处方率,并揭示其与长期生存的关系。这是一项基于前瞻性队列研究的模拟试验,受试者为2004年1月1日至2007年12月31日期间在以色列7个心胸科病房接受择期或半择期孤立性CABG手术的患者,并随访至2020年12月31日。 -导致死亡。 968 名患者 (n=573) 中只有 59.2% 在 CABG 手术后按 GDMT 出院。入院时使用 GDMT 使出院 GDMT 处方的可能性增加 7 倍(比值比,7.07;95% CI,5.04 至 9.91;<.001),未观察到性别差异。应用治疗加权的逆概率后,各组之间的基线特征得到了很好的平衡。在中位随访 13.7 年期间,采用倾向评分调整的治疗权重逆概率的 Cox 回归模型显示,接受 CABG 手术的出院 GDMT 处方患者的死亡率低于同行(风险比,0.75;95% CI) ,0.60 至 0.93;=.008)。手术前使用汇总 GDMT 使出院后更有可能接受 GDMT 处方,这反过来又与更好的长期生存相关。需要相关医疗专业人员开展教育工作,以尽量减少预防性治疗差距。 ClinicalTrials.gov 标识符:NCT00356863
更新日期:2024-03-07
中文翻译:
指南指导药物治疗的出院处方与冠状动脉搭桥手术后 15 年生存率的模拟试验
探讨冠状动脉搭桥术 (CABG) 术后指南指导药物治疗 (GDMT)(定义为聚合抗血小板药物、他汀类药物和 β 受体阻滞剂)的入院和出院处方率,并揭示其与长期生存的关系。这是一项基于前瞻性队列研究的模拟试验,受试者为2004年1月1日至2007年12月31日期间在以色列7个心胸科病房接受择期或半择期孤立性CABG手术的患者,并随访至2020年12月31日。 -导致死亡。 968 名患者 (n=573) 中只有 59.2% 在 CABG 手术后按 GDMT 出院。入院时使用 GDMT 使出院 GDMT 处方的可能性增加 7 倍(比值比,7.07;95% CI,5.04 至 9.91;<.001),未观察到性别差异。应用治疗加权的逆概率后,各组之间的基线特征得到了很好的平衡。在中位随访 13.7 年期间,采用倾向评分调整的治疗权重逆概率的 Cox 回归模型显示,接受 CABG 手术的出院 GDMT 处方患者的死亡率低于同行(风险比,0.75;95% CI) ,0.60 至 0.93;=.008)。手术前使用汇总 GDMT 使出院后更有可能接受 GDMT 处方,这反过来又与更好的长期生存相关。需要相关医疗专业人员开展教育工作,以尽量减少预防性治疗差距。 ClinicalTrials.gov 标识符:NCT00356863


























 京公网安备 11010802027423号
京公网安备 11010802027423号