Herz ( IF 1.7 ) Pub Date : 2024-03-11 , DOI: 10.1007/s00059-024-05241-6 Martin Möckel
|
The new guideline on acute coronary syndrome (ACS) of the European Society of Cardiology (ESC) replaces two separate guidelines on ST-elevation myocardial infarction (STEMI) and non-ST-elevation (NSTE) ACS. This change of paradigm reflects the experts view that the ACS is a continuum, starting with unstable angina and ending in cardiogenic shock or cardiac arrest due to severe myocardial ischemia. Secondary, partly non-atherosclerotic-caused myocardial infarctions (“type 2”) are not integrated in this concept.
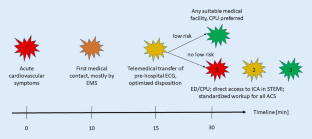
With respect to acute care in the setting of emergency medicine and the chest pain unit structures, the following new aspects have to be taken into account:
1. New procedural approach as “think A.C.S.” meaning “abnormal ECG,” “clinical context,” and “stable patient”
2. New recommendation regarding a holistic approach for frail patients
3. Revised recommendations regarding imaging and timing of invasive strategy in suspected NSTE-ACS
4. Revised recommendations for antiplatelet and anticoagulant therapy in STEMI
5. Revised recommendations for cardiac arrest and out-of-hospital cardiac arrest
6. Revised recommendations for in-hospital management (starting in the CPU/ED) and ACS comorbid conditions
In summary, the changes are mostly gradual and are not based on extensive new evidence, but more on focused and healthcare process-related considerations.
中文翻译:
新的 ESC 急性冠状动脉综合征指南及其对 CPU 和急诊科设置的影响
欧洲心脏病学会 (ESC) 关于急性冠脉综合征 (ACS) 的新指南取代了关于 ST 段抬高型心肌梗死 (STEMI) 和非 ST 段抬高型 (NSTE) ACS 的两个单独指南。这种范式的改变反映了专家的观点,即ACS是一个连续体,从不稳定心绞痛开始,以严重心肌缺血导致的心源性休克或心脏骤停结束。继发性、部分非动脉粥样硬化引起的心肌梗死(“2 型”)未纳入此概念。
关于急诊医学和胸痛科结构中的急性护理,必须考虑以下新方面:
1. 新的程序方法“认为 ACS”意味着“心电图异常”、“临床背景”和“表患者”
2. 关于体弱患者整体治疗方法的新建议
3. 关于疑似 NSTE-ACS 的影像学检查和侵入策略时机的修订建议
4. STEMI 抗血小板和抗凝治疗的修订建议
5. 心脏骤停和院外心脏骤停的修订建议
6. 院内管理(从 CPU/ED 开始)和 ACS 合并症的修订建议
总之,这些变化大多是渐进的,并不是基于广泛的新证据,而是更多地基于重点和医疗流程相关的考虑。


























 京公网安备 11010802027423号
京公网安备 11010802027423号