Current Cardiology Reports ( IF 3.7 ) Pub Date : 2024-03-16 , DOI: 10.1007/s11886-024-02032-7 Devinder S. Dhindsa , Wissam Mekary , Mikhael F. El-Chami
|
Purpose of Review
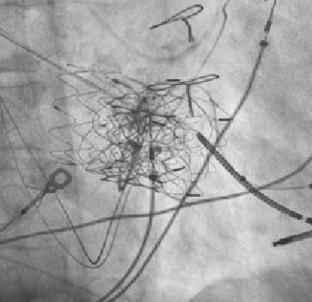
Tricuspid regurgitation is a commonly encountered valvular pathology in patients with trans-tricuspid pacing or implantable cardioverter-defibrillator leads. Transcatheter tricuspid valve interventions are increasingly performed in patients at high surgical risk. Implantation of these valves can lead to the “jailing” of a trans-tricuspid lead. This practice carries both short- and long-term risks of lead failure and subsequent infection without the ability to perform traditional transvenous lead extraction. Herein, this manuscript reviews available therapeutic options for lead management in patients undergoing transcatheter tricuspid valve interventions.
Recent Findings
The decision to jail a lead may be appropriate in certain high-risk cases, though extraction may be a better option in most cases given the variety of options for re-implant, including leadless pacemakers, valve-sparing systems, epicardial leads, leads placed directly through prosthetic valves, and the completely subcutaneous implantable-defibrillator.
Summary
A growing number of patients meet the requirement for CIED implantation in the United States. A significant proportion of these patients will have tricuspid valve dysfunction, either related to or independent of their transvenous lead. As with any percutaneous intervention that has shown efficacy, the role of TTVI is also likely to increase as this therapy advances beyond the investigational phase. As such, the role of the heart team in the management of these patients will be increasingly critical in the years to come, and in those patients that have pre-existing CIED leads, we advocate for the involvement of an electrophysiologist in the heart team.
中文翻译:
经导管三尖瓣置换术时代的起搏和除颤注意事项
审查目的
三尖瓣反流是使用经三尖瓣起搏或植入式心脏复律除颤器导线的患者中常见的瓣膜病变。经导管三尖瓣介入治疗越来越多地在手术风险较高的患者中进行。这些瓣膜的植入可能会导致经三尖瓣导线的“监禁”。这种做法存在短期和长期的导线失效和随后感染的风险,而无法进行传统的经静脉导线取出。在此,本手稿回顾了接受经导管三尖瓣介入治疗的患者铅管理的可用治疗方案。
最近的发现
在某些高风险病例中,监禁导线的决定可能是合适的,但在大多数情况下,鉴于重新植入的选择多种多样,包括无导线起搏器、瓣膜保留系统、心外膜导线、放置导线,拔除可能是更好的选择直接通过人工瓣膜和完全皮下植入式除颤器。
概括
在美国,越来越多的患者满足 CIED 植入的要求。这些患者中很大一部分会出现三尖瓣功能障碍,与其经静脉导线相关或无关。与任何已显示疗效的经皮介入治疗一样,随着该疗法进入研究阶段后,TTVI 的作用也可能会增强。因此,未来几年,心脏团队在这些患者的管理中的作用将变得越来越重要,对于那些已有 CIED 线索的患者,我们主张让电生理学家参与心脏团队。


























 京公网安备 11010802027423号
京公网安备 11010802027423号