Journal of Neuro-Oncology ( IF 3.9 ) Pub Date : 2024-03-23 , DOI: 10.1007/s11060-024-04633-2 Christoph Straube , Stephanie E. Combs , Denise Bernhardt , Jens Gempt , Bernhard Meyer , Claus Zimmer , Friederike Schmidt-Graf , Peter Vajkoczy , Arne Grün , Felix Ehret , Daniel Zips , David Kaul
|
Background
The optimal management strategy for recurrent glioblastoma (rGBM) remains uncertain, and the impact of re-irradiation (Re-RT) on overall survival (OS) is still a matter of debate. This study included patients who achieved gross total resection (GTR) after a second surgery after recurrence, following the GlioCave criteria.
Methods
Inclusion criteria include being 18 years or older, having histologically confirmed locally recurrent IDHwt or IDH unknown GBM, achieving MRI-proven GTR after the second surgery, having a Karnofsky performance status of at least 60% after the second surgery, having a minimum interval of 6 months between the first radiotherapy and the second surgery, and a maximum of 8 weeks from second surgery to the start of Re-RT.
Results
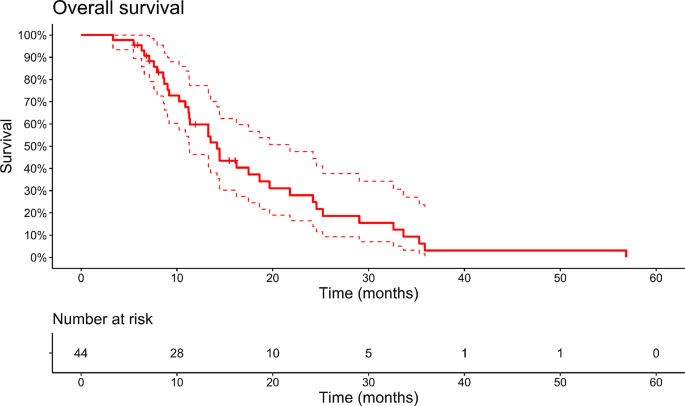
A total of 44 patients have met the inclusion criteria. The median OS after the second surgery was 14 months. All patients underwent standard treatment after initial diagnosis, including maximum safe resection, adjuvant radiochemotherapy and adjuvant chemotherapy. Re-RT did not significantly impact OS. However, MGMT promoter methylation status and a longer interval (> 12 months) between treatments were associated with better OS. Multivariate analysis revealed the MGMT status as the only significant predictor of OS.
Conclusion
Factors such as MGMT promoter methylation status and treatment interval play crucial roles in determining patient outcomes after second surgery. Personalized treatment strategies should consider these factors to optimize the management of rGBM. Prospective research is needed to define the value of re-RT after second surgery and to inform decision making in this situation.
中文翻译:
已切除的复发性胶质母细胞瘤的辅助再照射与不早期再照射:来自两个三级中心的汇总比较队列分析
背景
复发性胶质母细胞瘤(rGBM)的最佳治疗策略仍不确定,并且再照射(Re-RT)对总生存期(OS)的影响仍然存在争议。这项研究包括遵循 GlioCave 标准,在复发后进行第二次手术后实现全切除 (GTR) 的患者。
方法
纳入标准包括年满 18 岁或以上、经组织学证实局部复发 IDHwt 或 IDH 未知 GBM、第二次手术后达到 MRI 证明的 GTR、第二次手术后卡诺夫斯基功能状态至少为 60%、最小间隔时间为第一次放疗和第二次手术之间间隔 6 个月,从第二次手术到开始 Re-RT 最多间隔 8 周。
结果
共有 44 名患者符合纳入标准。第二次手术后的中位 OS 为 14 个月。所有患者在初次诊断后均接受标准治疗,包括最大安全切除、辅助放化疗和辅助化疗。 Re-RT 并未对 OS 产生显着影响。然而,MGMT 启动子甲基化状态和较长的治疗间隔(> 12 个月)与更好的 OS 相关。多变量分析显示 MGMT 状态是 OS 的唯一重要预测因子。
结论
MGMT 启动子甲基化状态和治疗间隔等因素在决定第二次手术后患者预后方面发挥着至关重要的作用。个性化治疗策略应考虑这些因素以优化 rGBM 的管理。需要进行前瞻性研究来确定第二次手术后再次放疗的价值,并为这种情况下的决策提供信息。


























 京公网安备 11010802027423号
京公网安备 11010802027423号