当前位置:
X-MOL 学术
›
J. Vasc. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Adoption and clinical outcomes of fenestrated endovascular aneurysm repair in a regional, multistate community hospital system
Journal of Vascular Surgery ( IF 4.3 ) Pub Date : 2024-03-01 , DOI: 10.1016/j.jvs.2024.02.030 Brant W. Ullery , Douglas Hanes , Eric B. Kirker , Kateri J. Spinelli
Journal of Vascular Surgery ( IF 4.3 ) Pub Date : 2024-03-01 , DOI: 10.1016/j.jvs.2024.02.030 Brant W. Ullery , Douglas Hanes , Eric B. Kirker , Kateri J. Spinelli
|
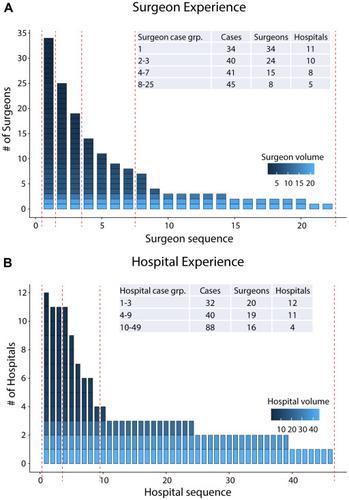
Complex endovascular abdominal aortic aneurysm (AAA) repair techniques have evolved over the last decade, yet patterns of physician and hospital system adoption of fenestrated endovascular aneurysm repair (FEVAR) remain poorly defined. We investigated clinical outcomes, use trends, and surgeon and hospital experience for FEVAR in a large community hospital system. We conducted a retrospective cohort study of all FEVAR procedures within our 5-state hospital system between April 2012 and June 2021. AAA repair volumes (open, EVAR, and FEVAR) were captured at the hospital and surgeon levels using Current Procedural Terminology and codes. Clinical and outcomes data were collected for FEVAR patients. To consider if surgeon or hospital experience influenced outcomes, sequential case number was used to divide patients into surgeon experience and hospital experience groups. Inverse probability weighted and generalized linear mixed models, adjusted for demographics and comorbidities, were built to examine risk-adjusted outcomes for surgeon and hospital experience groups. Of 3850 patients treated with AAA procedures of any kind between 2012 and 2021, 160 (4.2%) underwent FEVAR. FEVAR procedures were performed by 34 different surgeons at 12 hospitals, with intraoperative complications and unplanned adjunctive procedures occurring in 18.8% (n = 30) and 19.4% (n = 31) of patients, respectively. Among FEVAR patients, in-hospital mortality was 1.3% (n = 2) and postoperative morbidity was 16.9% (n = 27). Renal function decline occurred postoperatively in 5.1% of patients. Early (<30 day) postoperative endoleaks occurred in 15.3% of patients (n = 21). Target vessel patency was 95.6% on initial postoperative imaging. Surgeon and hospital experience had a small positive impact on outcomes after the first one to three cases. Significant decreases in operative time, fluoroscopy time, and estimated blood loss were observed with increased surgeon experience, relative to a surgeon's first case ( < .05). There were lower odds of intraoperative complications after a surgeon's first case (odds ratio [OR], 0.16; 95% confidence interval [CI], 0.03-0.77, for cases 2-3) or after a hospital's first one to three cases (OR, 0.19; 95% CI, 0.04-0.89, for cases 4-8; OR, 0.12; 95% CI, 0.03-0.55 for cases 9-49). Clinical outcomes of FEVAR across our hospital system compare favorably with previously published reports. Although system-wide FEVAR adoption increased 3-fold over the last decade, FEVAR continued to be performed by a minority of hospitals in our system. The results from this cohort demonstrate low rates of adverse events, high rates of technical efficiency, and a small impact of surgeon and hospital experience, thereby supporting this advanced endovascular technology as a safe, efficacious, and generalizable treatment alternative to open repair for patients with complex aortic anatomy.
中文翻译:

有窗血管内动脉瘤修复术在地区、多州社区医院系统中的采用和临床结果
复杂的腹主动脉瘤血管内修复技术在过去十年中不断发展,但医生和医院系统采用开窗血管内动脉瘤修复(FEVAR)的模式仍然不明确。我们调查了大型社区医院系统中 FEVAR 的临床结果、使用趋势以及外科医生和医院经验。我们对 2012 年 4 月至 2021 年 6 月期间 5 个州医院系统内的所有 FEVAR 手术进行了回顾性队列研究。使用当前手术术语和代码在医院和外科医生层面捕获了 AAA 修复量(开放、EVAR 和 FEVAR)。收集 FEVAR 患者的临床和结果数据。为了考虑外科医生或医院经验是否影响结果,使用连续病例数将患者分为外科医生经验组和医院经验组。建立逆概率加权和广义线性混合模型,根据人口统计和合并症进行调整,以检查外科医生和医院经验组的风险调整结果。 2012 年至 2021 年间,在 3850 名接受任何类型 AAA 手术治疗的患者中,160 名 (4.2%) 接受了 FEVAR。 FEVAR 手术由 12 家医院的 34 名不同外科医生进行,术中并发症和计划外辅助手术的发生率分别为 18.8% (n = 30) 和 19.4% (n = 31) 的患者。在 FEVAR 患者中,院内死亡率为 1.3% (n = 2),术后发病率为 16.9% (n = 27)。 5.1%的患者术后出现肾功能下降。 15.3% 的患者 (n = 21) 发生术后早期(<30 天)内漏。术后初次影像学检查靶血管通畅率为 95.6%。在第一到三个病例之后,外科医生和医院经验对结果产生了微小的积极影响。与外科医生的第一个病例相比,随着外科医生经验的增加,手术时间、透视时间和估计失血量显着减少 (< .05)。外科医生处理第一个病例后(病例 2-3 的比值比 [OR],0.16;95% 置信区间 [CI],0.03-0.77)或医院处理第一个到三个病例(OR ,0.19;对于病例 4-8,95% CI,0.04-0.89;OR,0.12;对于病例 9-49,95% CI,0.03-0.55)。我们医院系统的 FEVAR 临床结果优于之前发表的报告。尽管在过去十年中,全系统 FEVAR 的采用率增加了 3 倍,但我们系统中的少数医院仍然在执行 FEVAR。该队列的结果表明,不良事件发生率低,技术效率高,外科医生和医院经验的影响很小,从而支持这种先进的血管内技术作为一种安全、有效和普遍的治疗替代方案,可替代开放式修复术复杂的主动脉解剖结构。
更新日期:2024-03-01
中文翻译:
有窗血管内动脉瘤修复术在地区、多州社区医院系统中的采用和临床结果
复杂的腹主动脉瘤血管内修复技术在过去十年中不断发展,但医生和医院系统采用开窗血管内动脉瘤修复(FEVAR)的模式仍然不明确。我们调查了大型社区医院系统中 FEVAR 的临床结果、使用趋势以及外科医生和医院经验。我们对 2012 年 4 月至 2021 年 6 月期间 5 个州医院系统内的所有 FEVAR 手术进行了回顾性队列研究。使用当前手术术语和代码在医院和外科医生层面捕获了 AAA 修复量(开放、EVAR 和 FEVAR)。收集 FEVAR 患者的临床和结果数据。为了考虑外科医生或医院经验是否影响结果,使用连续病例数将患者分为外科医生经验组和医院经验组。建立逆概率加权和广义线性混合模型,根据人口统计和合并症进行调整,以检查外科医生和医院经验组的风险调整结果。 2012 年至 2021 年间,在 3850 名接受任何类型 AAA 手术治疗的患者中,160 名 (4.2%) 接受了 FEVAR。 FEVAR 手术由 12 家医院的 34 名不同外科医生进行,术中并发症和计划外辅助手术的发生率分别为 18.8% (n = 30) 和 19.4% (n = 31) 的患者。在 FEVAR 患者中,院内死亡率为 1.3% (n = 2),术后发病率为 16.9% (n = 27)。 5.1%的患者术后出现肾功能下降。 15.3% 的患者 (n = 21) 发生术后早期(<30 天)内漏。术后初次影像学检查靶血管通畅率为 95.6%。在第一到三个病例之后,外科医生和医院经验对结果产生了微小的积极影响。与外科医生的第一个病例相比,随着外科医生经验的增加,手术时间、透视时间和估计失血量显着减少 (< .05)。外科医生处理第一个病例后(病例 2-3 的比值比 [OR],0.16;95% 置信区间 [CI],0.03-0.77)或医院处理第一个到三个病例(OR ,0.19;对于病例 4-8,95% CI,0.04-0.89;OR,0.12;对于病例 9-49,95% CI,0.03-0.55)。我们医院系统的 FEVAR 临床结果优于之前发表的报告。尽管在过去十年中,全系统 FEVAR 的采用率增加了 3 倍,但我们系统中的少数医院仍然在执行 FEVAR。该队列的结果表明,不良事件发生率低,技术效率高,外科医生和医院经验的影响很小,从而支持这种先进的血管内技术作为一种安全、有效和普遍的治疗替代方案,可替代开放式修复术复杂的主动脉解剖结构。


























 京公网安备 11010802027423号
京公网安备 11010802027423号