
Abstract
The COVID-19 has placed pandemic modeling at the forefront of the whole world’s public policymaking. Nonetheless, forecasting and modeling the COVID-19 medical waste with a detoxification center of the COVID-19 medical wastes remains a challenge. This work presents a Fuzzy Inference System to forecast the COVID-19 medical wastes. Then, people are divided into five categories are divided according to the symptoms of the disease into healthy people, suspicious, suspected of mild COVID-19, and suspicious of intense COVID-19. In this regard, a new fuzzy sustainable model for COVID-19 medical waste supply chain network for location and allocation decisions considering waste management is developed for the first time. The main purpose of this paper is to minimize supply chain costs, the environmental impact of medical waste, and to establish detoxification centers and control the social responsibility centers in the COVID-19 outbreak. To show the performance of the suggested model, sensitivity analysis is performed on important parameters. A real case study in Iran/Tehran is suggested to validate the proposed model. Classifying people into different groups, considering sustainability in COVID 19 medical waste supply chain network and examining new artificial intelligence methods based on TS and GOA algorithms are among the contributions of this paper. Results show that the decision-makers should use an FIS to forecast COVID-19 medical waste and employ a detoxification center of the COVID-19 medical wastes to reduce outbreaks of this pandemic.
Similar content being viewed by others


1 Introduction
The prevalence of COVID-19 disease in recent months and the frequent visits to hospitals have led to an increase in the production of medical waste (Goodarzian et al., 2021b). As a simple comparison in Spain, medical waste, which includes surgical gloves, face masks, etc., with a significant increase of 350% in mid-March 2020, compared to the same period in 2019 by the waste agency Catalonia is registered. In Malaysia this number has increased to 27%, in China to 213% and in Iran the production of medical waste with outbreak of the COVID-19 disease to 17% (compared to the period from October 2019 to October 2020). Medical wastes contain a variety of microbial contaminants or chemical compounds or dressings and tissues and blood, and more recently, due to the spread of the Corona virus, the disposal of these wastes requires special attention. If the waste law is not managed properly and medical waste is disposed of properly, they can become the cause of disease and virus transmission.
The COVID-19 epidemic has created a global crisis and has increased economic and social problems in different countries of the world and has called for research in modelling resilience against pandemics, which have also spread to the issue of waste management and affected the management of municipal solid waste, especially processing and disposal (Sharma et al., 2020). For example, reducing the amount of municipal waste and increasing medical waste, as well as increasing the amount of recyclable and disposable waste in many cities around the world have been the consequences of this disease. Some countries have temporarily postponed their recyclable waste collection programs, and as a result, the amount of waste disposed of in some countries has increased (Goodarzian et al., 2021a).
Environmental health is an integral part of human health, and the COVID-19 pandemic is a global health challenge in the twenty-first century that has had a profound effect on the world economy and the health of the people, in a way that has greatly affected people’s lifestyles. One of its positive effects on the environment is the reduction of air pollution in many cities around the world, which led to the spontaneous reconstruction of nature and natural resources to provide an opportunity to analyze the accumulated pollutants in the environment. It was almost March 15, 2020, that a deadly virus called COVID-19 emerged and affected almost the entire world (Sharma et al., 2020). This virus is no exception to this and has caused positive and negative effects on the economy, society, environment, and so on. One of the measures taken by governments to eliminate or reduce its effects is to create restrictions and increase the distance between people, which has led to a decrease in industrial activity, car traffic, human activities, and so on. Thus, the positive environmental effects are evident including reduction of air pollution (through reduction of pollutants such as particulate matter with a diameter of 2.5 and 10 microns, nitrogen oxides, CO2), reduction of greenhouse gas emissions, reduction of river and sea pollution, reduction of noise pollution, reduction The volume of municipal and public solid waste and negative effects such as increasing the concentration of O3, SO2, increasing pollution of water resources through the penetration of disinfectants, increasing the volume of hospital waste and infectious household waste can be mentioned. There is also evidence of the influence of environmental factors (temperature, humidity, etc.) on the coronavirus. In general, coronavirus has caused positive environmental effects, and sustainability strategies have been proposed to maintain these conditions (Shadkam, 2021).Kindly check and confirm the Figures are renumbered for the sequentailly oder.checked and confirmed
A sustainable supply chain concentrates three-pillar including economic effects, environmental aspects, and social roles which sustainable concerns receiving raising attention during the COVID-19 epidemic. The COVID-19 epidemic presents more evidence which the three-pillar of sustainability are inextricably joined (Alkahtani et al., 2021). The issue of the COVID-19 epidemic effect on the sustainable supply chain is discussed worldwide. The COVID-19 epidemic causes modification in the lives of people worldwide as well as sustainability. The governments of all countries have performed actions that have led to the stop of transport and industrial activities to avoid people from meeting (Melin et al., 2021).
Since coronavirus is as a pandemic, this virus causes a global crisis that influences the world economy, human health, and the production of the COVID-19 medical waste. The COVID-19 crisis has made high fluctuation in the production of the COVID-19 medical waste (Mishra et al., 2021). Moreover, in the corona crisis, the production of medical wastes is getting out of control. In order to provide a proper strategy for COVID-19 diseases, the requirement to forecast the number of the COVID-19 medical wastes and the allocation of the COVID-19 detoxification center is becoming acutely significant and considerable. Then, no papers have evaluated the related to the forecast the COVID-19 medical waste as well as allocation and location of the detoxification center in Iran to the best of knowledge. Thus, this paper’s goal is to design a COVID-19 predicting system to control the spread, manage the situation, and understand the situation in time (Melin et al., 2021).
In this paper, a new sustainable COVID-19 medical waste supply chain network for allocation and location of the detoxification center of the COVID-19 medical wastes is designed for the first time. Then, the fuzzy inference system to predict the COVID-19 diseases is employed. Also, people are divided into four groups containing healthy people, suspicious, suspected of mild COVID-19, and suspicious of intense COVID-19. In the mathematical model, disposal centers, potential location for temporary detoxification centers, and existing detoxification centers simultaneously are considered for the first time. To solve the proposed model, a new heuristic method based on TS and GOA algorithms called MGOTSA is developed for the first time. Finally, a real case study is suggested in Iran to show the performance and efficiency of the proposed problem.
The rest of the proposed research is organized as follows. The literature review is stated in Sect. 2. In Sect. 3, the problem description, fuzzy inference system, and mathematical modeling are explained. The solution method is surveyed in Sect. 4. Case study and computational results are addressed in Sects. 5 and 6 respectively. Eventually, the conclusion, and future work are explained in the last section.
2 Literature review
In this section, the studies related to the forecasting COVID-19, waste management, mathematical model during the COVID-19 epidemic are examined.
Ly, (2020) provided the system of the COVID-19 forecasting based on adaptive neuro-fuzzy inference to predict the COVID-19 patient numbers in UK. Also, in order to provide an efficient time series prediction model, they evaluated the different agents of adaptive neuro-fuzzy inference system. Finally, they indicated that Italy and Spain data can be amplified the predictive vigor of COVID-19 patient numbers in UK.
Sarkar et al. (2020) presented a mathematical model for predicting the COVID-19 dynamics in India. In order to show ending phase of SARS-CoV-2 and the predicted inflection point, a complete scenario was provided to indicate the estimated epidemic life cycle. The dynamic monitors in their model were divided into six categories including asymptomatic, quarantined susceptible, infected, isolated infected, susceptible, and recovered. They performed a set of sensitivity analysis to analysis the predicted power of their model to the values of the parameter. According to the sensitive parameters, they estimated the real data related to the COVID-19 epidemic. Al-Qaness et al. (2020) developed an improved adaptive neuro-fuzzy inference system according to the salp swarm algorithm and an enhanced flower pollination approach. According to the World Health Organization official information of the COVID-19 pandemic, the improved system was assessed to predict the confirmed patients. Therefore, in terms of the Root Mean Squared Relative Error, coefficient of determination, computational time, and Mean Absolute Percentage Error, the improved system had better efficiency compared with some available models. Finally, to validate their system and model, two real case studies in the USA and China were considered. Behnood et al. (2020) developed a novel approach according to a hybrid adaptive network-based fuzzy inference system and the virus optimization algorithm. Their developed method was utilized to evaluate the effects of population density and climate-related agents on the spread of the COVID-19. Eventually, they suggested a real case study in the USA. Maleki et al. (2020) considered time series models for the COVID-19 data. Then, they displayed the distribution of the error to be two-piece scale mixtures of normal. Eventually, they selected their models based on the forecast of the death rate of COVID-19 and the number of confirmed cases. Ahmad et al. (2021) provided a sustainable production and waste management of COVID-19 medical equipment under uncertainty. They used the intuitionistic fuzzy method to cope with uncertain parameters. In addition, they recommended a real case study in an Indian automobile company to show the better waste management.
In this regards, Shaban et al. (2021) introduced a novel hybrid diagnose technique. In addition, they provided a hybrid model according to a deep neural network and fuzzy inference engine. To validate obtained results, Friedman Test and Wilcoxon Signed Rank Test was used. Nikolopoulos et al. (2021) developed a novel hybrid predicting approach according to the clustering and nearest neighbors. They predicted the rates of the COVID-19 growth based on epidemiological, machine- and deep-learning, and statistical models. They employed simulating governmental decisions (lockdown) and auxiliary data (google trends) to predict the excess demand for services and products in the COVID-19 epidemic. Melin et al. (2021) employed the firefly algorithm for the optimization of the neural network to forecast the COVID-19 time series. Then, they suggested type-2 fuzzy logic in a weighted average integration approach. Finally, the firefly algorithm was designed for an ensemble neural network architecture in each one of 26 countries.
Goodarzian et al. (2021a) designed an integrated multi-objective, multi-level, multi-product, and multi-period sustainable medical supply chain network during the COVID-19 epidemic. They provided a production–distribution–inventory–allocation–location problem in the proposed network. They used meta-heuristic algorithms called firefly, fish swarm, and ant colony optimization algorithms and developed three new meta-heuristic algorithms, namely, hybrid VNS along with the proposed algorithms to solve their model. To tune and control the algorithm’s parameters, the response surface approach was employed. Finally, a real case study in Iran was suggested. Karmaker et al. (2021) investigated sustainable supply chain drivers to tackle with the disruptions of the supply chain during the COVID-19 condition. They provided a novel solution method according to the fuzzy theory, Matriced Impacts Cruises Multiplication Applique a un Classement, Pareto analysis, and total interpretive structural modeling methods. Then, their presented method experimented with utilizing academic experts’ inputs from the emerging economy and experienced supply chain practitioners. Finally, they suggested a real case study in Bangladesh. Alkahtani et al. (2021) formulated a non-linear supply chain network model considering the rate of controllable production. Then, their main aims were to optimize the whole cost of production and to cope with the various conditions under variable demand. Therefore, to cope with uncertain parameters such as costs, the fuzzy approach was utilized. To solve their model, they provided numerical test problems. Finally, the results indicated that to tackle the emergencies in an epidemic, the decision-makers according to the proactive plan through the optimal usage of the rate of the resources and controllable production was supported. Foy et al. (2021) designed a novel mathematical model of the COVID vaccine allocation strategies utilizing an SEIR model. They considered an age-structured and expanded SEIR model with social contact matrices. Also, according to the prioritizing various age groups, they suggested a simulation approach to survey the relative decreasing in morbidity and mortality. They varied vaccine features in the modeling simulations according to the uncertainty related to the production of the COVID-19 vaccine. Finally, they suggested a real case study in India for the efficiency of their model.
In terms of the waste management, Sharma et al. (2020) presented specific cases for biomedical waste, plastic waste, and food waste management. They investigated challenges, opportunities, and innovations for effective solid waste management during and post COVID-19 epidemic. Shadkam, (2021) formulated an integer linear programming model in the reverse logistic network for COVID-19 waste management. Their main aim was to minimize the costs related to the fixed costs, material flow costs, and the costs of building potential centers. Accordingly, they used the Cuckoo optimization algorithm to solve their model. Mishra et al. (2021) presented a mathematical model for selecting drugs for the treatment of Covid-19. The considered uncertainty is fuzzy and the additive ratio assessment and Hesitant Fuzzy Sets (HFS) approaches have been used to select drugs. The considered case study was the influenza outbreak in Japan. The results obtained by the divergence measure indicate that the proposed algorithm performed well. Si et al. (2021) presented a probabilistic mathematical model to explore neutral membership grade using Dempster–Shafer theory and grey relational analysis. They have applied their model to solve the COVID-19 medicine selection problem. They have compared the proposed method with the three methods and results show the superior of their proposed model. Goodarzian et al. (2021b) developed a sustainable-resilient health care network during the COVID-19 epidemic under uncertainty. In addition, they provided a multi-period, multi-product, multi-objective, and multi-echelon mixed-integer linear programming model for production, allocation, location, inventory holding, distribution, and flow decisions. They used hybrid meta-heuristic algorithms to solve their model. Finally, they suggested a real case study in the United States to validate their problem. Melin et al. (2022) proposed a method called ENNT3FL-FA that combines ensemble neural networks and type-3 fuzzy inference systems to predict COVID-19 data for confirmed cases in 12 countries. The method seeks to find the best possible parameters for each module of the ENN and the type-3 FIS. The results showed that the proposed method allows for better predictions of future confirmed cases, especially when the number of data points increases. Castillo et al. (2022) proposes an approach for fuzzy aggregation in ensembles of neural networks to improve forecasting by combining the outputs of the networks in a weighted average calculation. A fuzzy system was used to estimate the weights assigned to the outputs, and interval type-3 fuzzy was used to model the uncertainty in the aggregation process, showing potential to outperform other aggregators in the literature when tested on COVID-19 data sets.
According to the examined papers in the literature review, research gaps are extracted as follows:
-
Lack of attention to the amount of medical wastes during the COVID-19 pandemic,
-
Lack of attention to the classification of people into different groups which in the most studies have considered only patients,
-
Lack of attention to sustainability in COVID 19 medical waste supply chain network
-
In the examined studies, location and distribution decisions of the COVID-19 medical wastes simultaneous were not considered.
-
In the examined papers did not use the artificial intelligence methods based on TS and GOA algorithms called MGOTSA, but the developed method is used for solving the proposed model for the first time in this paper.
The main contributions of paper as follows:
-
Estimating the amount of medical wastes during the COVID-19 pandemic using fuzzy inferences system,
-
Classifying of people into different groups based on their disease history,
-
Considering sustainability in COVID 19 medical waste supply chain network
-
Determining the location and distribution decisions of the COVID-19 medical wastes simultaneous.
-
Presenting a new heuristic approach based on artificial intelligence methods, namely, the Grasshopper Optimization Algorithm and Tabu Search algorithm called Modified Grasshopper Optimization Algorithm and Tabu Search is developed
3 Problem description
In this study, the amount of hospital waste of the COVID-19 patient is estimated using a Fuzzy Inference System (FIS). The way it process is that first the inputs and outputs of the inference system are defined. Inputs include questionnaires about the percentage of blood oxygen in people, the number of days of dry cough, the number of days of fever, the number of days of headache and body aches, and the loss of smell or taste. In this regard, the output of the system includes the classification of people into five types. These five categories are divided according to the symptoms of the disease into healthy people, suspicious, suspected of mild COVID-19, and suspicious of intense COVID-19. After determining the inputs and outputs, membership functions are determined for each, which shows the degree of dependence of people on inputs and outputs. After defining the groups, it is time to determine the fuzzy rules. These rules have been extracted by experts, infectious disease physicians and based on patient examination. Hence, the amount of hospital waste of the COVID-19 patient is determined according to the assigned group after determining the groups by the fuzzy inference system. The point is that first the number of COVID-19 patients is estimated, and then the amount of medical wastes will be calculated based on the number of patients. Then, the outputs are defuzzied and injected to the mathematical model as a “waste generated by the hospital” parameter.
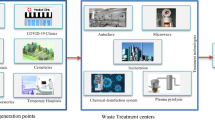
The main purpose of the proposed mathematical model is to minimize supply chain costs, the environmental impact of medical waste, and to establish detoxification centers and control the social responsibility centers in the COVID-19 outbreak. In the proposed network, hospitals send medical waste to existing and established detoxification centers. Detoxification centers are used to detoxify medical waste. This prevents the possibility of re-infection of the COVID-19 virus through waste. According to the increase in the production of infectious waste under the conditions of COVID-19 is obvious, the existing detoxification centers do not meet the high demand. Therefore, temporary detoxification centers are located in this study. The detoxified waste is transported to landfills. Figure 1 shows the proposed medical waste supply chain network structure.

The structure of the proposed network in this paper
Finally, the sensitivity analysis of the proposed model and the fuzzy inference system is performed. Figure 2 indicates the framework of the presented research.

The structure of an FIS
3.1 Fuzzy inference system
In order to design an FIS, first of all Fuzzifier, meaning the receipt of inputs and determining their membership to each of the fuzzy sets is performed through membership functions. Then, the rule base is designed and finally, the fuzzy output will be converted to a deterministic number. The process of converting explicit variables to linguistic variables is called Fuzzifier. The inference engine assesses and inferred the rules utilizing inference algorithms, and after the aggregation of the output rules by the Defuzzified unit, it becomes an explicit or numerical value. Then, Fig. 3 demonstrates the structure of the FIS. There are several advantages of using a fuzzy inference system (FIS) to forecast the amount of medical waste generated due to the COVID-19 pandemic. Here are some of the key advantages:
-
Handles uncertainty and imprecision: FIS is well-suited to handle uncertainty and imprecision in the input data. This is important in the context of COVID-19 medical waste forecasting because there is often incomplete or uncertain data available about the number of cases and the amount of waste generated.
-
Flexibility: FIS can be easily adapted and updated to reflect changes in the input data or the environment. This is important in the context of COVID-19 because the situation is constantly evolving, and the amount of waste generated may change as the pandemic progresses.
-
Handles complex relationships: FIS can handle complex nonlinear relationships between input variables and output variables. This is important in the context of COVID-19 medical waste forecasting because there may be complex relationships between the number of cases, the population, and the amount of waste generated.

The framework of the presented research
The FIS design process consists of four phases as follow:
-
Phase 1
A fuzzifier at the input that converts the numeric value of the variables into a fuzzy set:
In this step, the membership function is defined for each input. The membership function considered in this study is triangular. Figure 4 displays the membership function of this research.

The membership function of this research
-
Phase 2
A fuzzy rule database that is a set of if–then rules:
An if–then rule is defined as “if x is equal to A, then Y is equal to B”, where x and Y are the input and output variables, and A and B are the membership functions written for these variables.
-
Phase 3
Fuzzy inference engine that converts inputs to output with a series of operations:
-
Application of fuzzy operators: In this step, Mamdani fuzzy operator is employed in Eq. (1) as follows:
$$R\left( {U,V} \right) = {\text{min}}\left[ {\mu_{A} \left( u \right),\mu_{B} \left( u \right)} \right]$$(1)
In the following, the weight of each rule is determined by the expert or any method, must be multiplied by accuracy coefficient of rule, then applied to the output function. Finally, the aggregation of the outputs is performed. There are different methods for aggregation. The most important include Max and Sum, which in this study, the Sum method is used.
-
Phase 4
Defuzzifier that converts the fuzzy output to a deterministic number:
In this research, the center of gravity method is used for defuzzy, which Eq. (2) shows defuzzy according to the center of gravity.
Input and output information for the fuzzy inference system is obtained from the Ministry of Health of Iran, medical experts, and the WHO. For this purpose, the COVID-19 patients are divided into four general categories that report in Table 1.
The designed FIS can estimate the amount of medical waste. How the decision support system works is as follows:
First, the number of COVID-19 patients is estimated, and then the number of medical waste is estimated according to the number of people infected and hospitalized. Therefore, the criteria for measuring the health of people in the COVID-19 condition are determined based on WHO. These criteria include (1) The percentage of oxygen in the blood of people, (2) Dry cough, (3) Fever, (4) Headache and body ache, and (5) Loss of smell or taste. Therefore, the five mentioned criteria are considered as input variables of the FIS. Then, the inputs are entered into the system as a low, mid, and high membership function. For example, the percentage of oxygen between 95 and 99 is known as high, between 90 and 94 as mid and below 90% is known as low. Also, if the number of days a person has a fever is 1 day, it is known as low, if it is between 1 to 3 days, it is known as mid, and more than 3 days, it is known as high. Therefore, the output of the FIS as a membership function is shown in Table 2.
Next, the rules of the inference system are entered into the inference system by experts and physicians based on the patient’s condition. It should be noted that different rules can be entered into the system based on each group. Finally, all the information of the people, including the study, is entered into the inference system. These people should answer questions about blood oxygen levels, the number of days they have a fever, headache, body aches, and dry cough. They are also asked about the loss of taste and smell. After entering the information, it is determined to which type each person belongs. The amount of medical waste in hospitals is estimated based on which person belongs to which type. After estimating the amount of medical wastes, this information is entered into the mathematical model, and logistical programming is performed for the medical wastes.
3.2 Mathematical model
In this subsection, the assumptions of the proposed medical waste supply chain model are provided.
-
The model is considered as multi-objective, multi-period, and multi-echelon.
-
Temporary detoxification center is considered as potential and the optimal location of the temporary detoxification center is selected from the potential locations.
-
The capacity of detoxification centers for detoxification is limited.
-
The amount of waste generated by the hospital is considered fuzzy and this parameter is estimated by the fuzzy inference system.
In the following, the indices, parameters, and decision variables are explained.
Indices | |
|---|---|
\(h\) | Hospitals |
\(d\) | Disposal centers |
\(l\) | Potential location for temporary detoxification centers |
\(e\) | Existing detoxification centers |
\(t\) | Periods |
Parameter | |
\({cb}_{d}\) | Unit burial cost in disposal center \(d\) |
\({cd}_{e}\) | Unit detoxification cost in existing detoxification center \(e\) |
\(cd{\prime }_{l}\) | Unit detoxification cost in temporary detoxification center \(l\) |
\(p_{he}\) | Population density between hospital \(h\) to existing detoxification center \(e\) |
\(p{\prime }_{hl}\) | Population density between hospital \(h\) and temporary detoxification center \(l\) |
\(p{\prime \prime }_{e}\) | Population density around the existing detoxification center \(e\) |
\(p{\prime \prime \prime }_{l}\) | Population density around the temporary detoxification center \(l\) |
\(s_{h}\) | The weight determines the severity of the hazardous waste in the hospital \(h\) |
\(tc_{he}\) | Transportation cost of a unit medical waste from hospital \(h\) to existing detoxification center \(e\) |
\(tc{\prime }_{hl}\) | Transportation cost of a unit medical waste from hospital \(h\) to temporary detoxification center \(l\) |
\(tc{\prime \prime }_{ed}\) | Transportation cost of a unit medical waste from existing detoxification center \(e\) to disposal center \(d\) |
\(tc{\prime \prime \prime }_{ld}\) | Transportation cost of a unit medical waste from temporary detoxification center \(l\) to disposal center \(d\) |
\(cs_{l}\) | Setup cost of temporary detoxification center \(l\) |
\(oc_{l}\) | Fixed operating cost of temporary detoxification center \(j\) |
\(oc{\prime }_{e}\) | Fixed operating cost of existing detoxification center \(e\) |
\(ca_{e}\) | Capacity of existing detoxification center \(e\) |
\(ca{\prime }_{l}\) | Capacity of temporary detoxification center \(l\) |
\(ec_{l}\) | Establishment cost of temporary detoxification center \(l\) |
\(gw_{ht}\) | The amount of waste generated by the hospital \(h\) in period \(t\) |
\(rm_{he}\) | Risk of medical waste transportation between hospital \(h\) and existing detoxification center \(e\) |
\(rw_{hl}\) | Risk of medical waste transportation between hospital \(h\) and temporary detoxification center \(l\) |
\(rp_{l}\) | Risk of medical waste detoxification in temporary detoxification center \(l\) |
\(re_{e}\) | Risk of medical waste detoxification in existing detoxification center \(e\) |
\(ke_{e}\) | Amount of CO2 emission (per kilogram) which is released in existing detoxification center \(e\) |
\(ke{\prime }_{l}\) | Amount of CO2 emission (per kilogram) which is released in temporary detoxification center \(l\) |
\(kp_{he}\) | Amount of CO2 emission (per kilogram) which is released between hospital \(h\) to existing detoxification center \(e\) |
\(kp{\prime }_{hl}\) | Amount of CO2 emission (per kilogram) which is released between hospital \(h\) and temporary detoxification center \(l\) |
\(kp{\prime \prime }_{ld}\) | Amount of CO2 emission (per kilogram) which is released temporary detoxification center \(l\) and disposal center \(d\) |
\(kp{\prime \prime \prime }_{ed}\) | Amount of CO2 emission (per kilogram) which is released between existing detoxification center \(e\) and disposal center \(d\) |
Decision variables | |
\({w}_{et}\) | 1 If existing detoxification center \(e\) is utilized in period \(t\), 0 otherwise |
\({es}_{l}\) | 1 If temporary detoxification center \(l\) is established, 0 otherwise |
\({z}_{lt}\) | 1 If temporary detoxification center \(l\) is utilized in period \(t\), 0 otherwise |
\({y}_{hlt}\) | Amount of medical waste transported from hospital \(h\) to temporary detoxification center \(l\) in period \(t\) |
\({x}_{het}\) | Amount of medical waste transported from hospital \(h\) to existing detoxification center \(e\) in period \(t\) |
\({n}_{lt}\) | The amount of medical waste detoxified at temporary detoxification center \(l\) in period \(t\) |
\({m}_{et}\) | The amount of medical waste detoxified at existing detoxification center \(e\) in period \(t\) |
\({u}_{ht}\) | Amount of uncollected medical waste in the hospital \(h\) in period \(t\) |
\({a}_{edt}\) | Amount of medical waste transported from existing detoxification center \(e\) to disposal center \(d\) in period \(t\) |
\({b}_{ldt}\) | Amount of medical waste transported from temporary detoxification center \(j\) to disposal center \(d\) in period \(t\) |
Constraints:
Objective function (3) minimizes the total amount of costs in the proposed chain. These costs include fixed operating cost, detoxification cost in existing and existing detoxification center, setup cost, transportation costs, total burial costs and cost of establishing temporary detoxification centers. The objective function (4) controls social responsibility. Therefore, in this objective function, the transportation risks, detoxification and establishment of new centers is minimized. Accordingly, the first and second terms minimize detoxification risks and the third and fourth terms minimize transportation risks. The final term also tries to keep established centers as far away from densely populated areas as possible. Hence, the proposed model tries to reduce the possibility of establishing new centers in areas with more population. Objective function (5) minimizes the environmental impact under COVID-19 condition. Thus, this objective function minimizes the amount of carbon dioxide released due to detoxification, transportation and the establishment of new centers.
Constraints (6) and (7) specify the amount of medical waste detoxified at existing and temporary detoxification centers. Constraint (8) controls the balance of transported medical waste between hospitals and temporary and existing detoxification centers. Constraints (9) and (10) show the capacity of medical waste in temporary and existing detoxification centers. Constraints (11) and (12) indicate that all detoxified medical waste in existing and temporary detoxification centers must be transferred to landfills. Constraint (13) describes the type of decision variables of the proposed mathematical model.
4 Solution methodology
In this section, artificial intelligence methods based on meta-heuristic algorithms are developed to obtain the best solution and optimal Pareto solution (Towell & Shavlik, 1994). Accordingly, two meta-heuristic algorithms called the grasshopper optimization algorithm (GOA) and the Tabu Search (TS) algorithm are presented to obtain near-optimal solutions. Additionally, a new heuristic method called Modified Grasshopper Optimization Algorithm and the Tabu Search (MGOTSA) is developed to solve the sustainable COVID-19 medical waste supply chain problem for the first time. In the following, the structure of the suggested algorithms is explained.
4.1 Grasshopper optimization algorithm
One of the newest optimization algorithms presented by Saremi et al. (2017) is the Grasshopper Optimization Algorithm (GOA). The GOA is a nature-inspired meta-heuristic that mimics and simulates the behavior of grasshoppers in nature and the group movement of grasshoppers toward food sources. Although grasshoppers are usually seen alone and separately in nature, they belong to one of the largest groups of all creatures. The size of the groups can be very large. In fact, grasshoppers in nature have a pattern of behavior when they live in groups to find food, which includes two stages: exploitation and exploration. In exploration, search agents are encouraged to make random moves, while in the exploitation stage; they tend to move locally and around their place.
The mathematical model of the GOA is an imitation of the behavior of grasshoppers in nature for solving the optimization problem. The simulation outcomes indicate that the GOA is able to propose superior outcomes in comparison with the examined algorithms in the literature. The simulation outcomes on real problems also proved that the GOA is able to solve real problems with unknown space. Hence, for the details related to the GOA, interested scholars can read to (Saremi et al. (2017); Dinh, (2021)) references. Then, the pseudocode of the GOA is indicated in Fig. 5.

The pseudocode of the GOA algorithm
4.2 Tabu search algorithm
The TS is a meta-heuristic optimization algorithm introduced for the first time by Glover, (1986). To get the optimal solution to an optimization problem, the TS algorithm begins from an initial solution. Hence, the TS selects the best neighbor answer from between the current answer neighbors. If this answer is not in the Tabu list, the TS moves to the neighboring answer; otherwise, the algorithm will check a measure, namely, the measure of respiration. According to the measure of respiration, if the neighbor’s answer is better than the best answer ever found, the algorithm will move to it, even if that answer is in the Tabu list. After the algorithm moves to the neighbor’s answer, the Tabu list is updated. This means that the previous move by which we moved to the neighbor’s answer is placed in the Tabu list to prevent the algorithm from returning to that answer and creating a cycle. In fact, the Tabu list is a tool in the TS that prevents the algorithm from being optimally located locally. After placing a previous move on the Tabu list, a number of moves that were previously on the Tabu list will be eliminated from the list. The length of time that movements are on the Tabu list is specified by a parameter called Tabu tenure. The move from the current answer to the neighbor’s answer continues until the termination condition is met. Then, interested researchers can refer to (Chou et al. (2021)) for more details about the TS algorithm. Therefore, the pseudocode of the TS is shown in Fig. 6.

The pseudocode of the TS algorithm
4.3 Heuristic approach (MGOTSA)
According to the poor exploitation and exploration, the GOA algorithm gets stuck in local optima. In this paper, a neighbor method from the TS algorithm is incorporated for the achieved the best solution from the main loop of the GOA in each iteration to modify the performance of GOA. For this reason, the heuristic approach reaches a promising region within the defined boundary, causes speed-up convergence, and makes this method more feasible for a wider range of real-world applications. Then, the structure steps of the MGOTSA algorithm are illustrated in Fig. 7 and the pseudocode of the MGOTSA is indicated in Fig. 8.

The pseudocode of the MGOTSA algorithm

The flowchart of the MGOTSA steps
5 Numerical examples
In this section, first of all, the generated data is explained to investigate the efficiency of proposed algorithms. Hence, to tune the algorithm’s parameter, the Taguchi method is used. Finally, speed convergence, assessment metrics, and computational time (CPU) are employed to compare of the presented algorithms. The proposed artificial intelligence methods are implemented on MATLAB 2020b Software.
5.1 Generated data
In this sub-section, generated data divided into two test problems including small- and medium-sized. Additionally, large-sized problems are related to the case study. Therefore, the size of the test problems is shown in Table 3 and the range of the proposed parameters is shown in Table 4.
5.2 Taguchi method
Since the suggested algorithms have a set of parameters, the Taguchi approach is utilized to tune and control the algorithm’s parameters. A few of recent papers are offered to see the details of this method e.g., (Goodarzian et al., 2021b). The characteristics of comparison are divided into two main groups in the Taguchi method: the factors of the control and noise. This approach uses to compute the value of response variation according to Signal to Noise (S/N) ration. Hence, the mechanism of this approach depends on the answer type. That’s mean the presented solution related to each group of Taguchi classification groups: smaller is better, larger is the better type, and the nominal is better. Since the presented solution of the proposed research is maximization type, “the larger is better type” is used to tune of each algorithm’s parameters. In Eq. (14), the value of the S/N ratio is formulated.
where \(x_{j}\) illustrates the value of the solution for \(j\) th orthogonal array as well as \(m\) shows the number of orthogonal arrays.
In this paper, GOA, TS, and MGOTSA algorithms are suggested. Accordingly, the levels and factors of the proposed algorithms are reported in Table 5. Taguchi approach utilizing Orthogonal Arrays (OA) has greatly decreased the number of tests. These arrays are selected with special features from the total number of tests in the complete factorial approach. Therefore, this approach suggests L9 for GOA and TS as well as L27 for MGOTSA that show in Tables 6 and 7 respectively.
Thus, the output of S/N ratio analysis through Minitab Software to find the best levels of each proposed algorithm (see Figs. 9, 10 and 11).

The output of the S/N ratio for GOA

The output of the S/N ratio for TS

The output of the S/N ratio for MGOTSA
Then, the CPLEX approach, two methods (GOA and TS), and a heuristic method (MGOTSA) are suggested to solve the test problems. Table 8 shows the outputs of the objective functions and computational (CPU) time. Figure 12 indicates the behavior of CPU time of the presented approaches in small- and medium-sized problems.

The behavior of CPU time of the suggested artificial intelligence methods in small- and medium-sized
According the results of the objective functions in small-sized, with increasing problem size, the outcomes of CPLEX are increased, and CPU Time also is increased. But, CPU Time of other methods are less than CLPEX. Therefore, CPLEX method is not suitable for medium- and large-sized problems. Therefore, metaheuristic algorithms are used for medium-sized problems. To comparison between the mentioned algorithms, MGOTSA has less CPU Time. It shows that this algorithm has a good performance and efficiency (see Table 8 and Fig. 12).
5.3 Assessment metrics to compare of the proposed algorithms
In this paper, various efficiency assessment metrics are suggested to compare the quality of obtained non-dominated solutions by suggested algorithms. Here, two assessment metrics are employed to compare the performance of the proposed meta-heuristics including (\(i\)) Number of Pareto Solutions (NPS) computes the total non-dominated solutions acquired by an algorithm (more is better) and (\(ii\)) Mean Ideal Distance (MID) shows the distance among non-dominated solutions and ideal point (less is better). Thus, the assessment metrics are computed according to the attained Pareto front for all the proposed test problems to evaluate the performance of each meta-heuristic are shown in Table 9.
Moreover, an instance of non-dominated solutions of suggested algorithms in two test problems (S3 and M3) are shown in Fig. 13. It is clear that MGOTSA indicates the best efficiency, but TS shows the worst performance.

Pareto frontier of suggested algorithms in S3 a and M3 b
Therefore, some statistical comparisons between the proposed meta-heuristics according to the assessment metrics are performed to decisively find out which meta-heuristic has high quality and more performance. In this paper, based on Relative Deviation Index (RDI) is conducted statistical comparisons between the proposed meta-heuristics. It should be noted that the lower value of RDI is better. Therefore, the confidence interval of 95% for the assessment metrics in the proposed meta-heuristics is conducted to statistically analyze effectiveness of meta-heuristics. Figure 14 presents the means plot and LSD intervals for the suggested meta-heuristics.

Means plot and LSD intervals for the proposed meta-heuristics in a NPS and b MID
Accordingly, in terms of the NPS metric, while there is no statistically significant difference among proposed algorithms, but MGOTSA is more efficient than the GOA and TS algorithms in Fig. 14a. Additionally, as demonstrated in Fig. 14b, based on the results of the MID, there are some overlaps between the proposed meta-heuristics. In this regard, MGOTSA algorithm high priority over the proposed algorithms.
6 Case study
The city of Tehran with a population of more than 9 million is one of the most populous metropolises in Iran and Asia. According to the received information from the Ministry of Health of Iran, as of 2021.01.06, 2,945,100 people have been infected with the COVID-19 virus, of which 80,658 have died. The period of obtained information in the case study was the first 5 months of 2021. There are 17 detoxification centers (7 existing center and 10 temporary center), 8 disposal centers and 15 hospitals in Tehran. Hospitals deliver medical wastes to detoxification centers at different times. The main concern of decision-makers is to estimate the medical waste demand and the location of temporary detoxification centers in Tehran. Also, amount of uncollected medical waste in the hospital and the amount of medical wastes flow between hospitals, detoxification centers and disposal centers in Tehran have been studied. Figure 15 illustrates a real case study map of the proposed paper.

The map of the case study
Table 10 reports the capacity of existing and temporary detoxification center in the first period. Additionally, Table 11 shows the severity of the hazardous waste in the hospitals in the first period.
7 Computational results
The relevant codes were implemented in MATLAB R2020b v9.9.0.1495850, LINGO 17.0.0.78 software. The proposed case study was run on a computer with an Intel Core i5-8250U 1.60 GHz CPU and 8 GB RAM. The results are explained as follows:
7.1 Fuzzy inference system results
Figure 16 shows the input and output structure of the designed fuzzy inference system. The number of considered rules is equal to 130 rules and all rules are from AND type. The desired output of the amount of medical waste generate by each group is defined for five groups. Figure 17 indicates the range of output variables in terms of the amount of input data.

The input and output structure of the designed fuzzy inference system

Membership functions of output variables
Table 12 illustrates the twenty generated rules by the fuzzy inference system in terms of the inputs and outputs in Fig. 16. For example, it is clear that in User 1, the blood oxygen level is Mid (between 90 and 94), the duration of dry cough is equal to 11, the duration of fever is equal to 9, and the sense of smell and taste is low level.
In addition, Table 13 reports the output values and results of the designed rules. For example, according to the extracted rules, the first law belongs to the first class and the second law belongs to the second class.
7.2 The results of the proposed mathematical model for case study
Table 14 shows the number of established distribution centers in the first period. As can be seen, after solving the mathematical model, temporary detoxification centers 2, 7, and 10 have not been established.
Table 15 demonstrates the amount of medical waste transported from temporary detoxification center to disposal center in the first period. It is clear that for example, 4180 KG medical waste transported from temporary detoxification center 1 to disposal center 8. Additionally, Table 16 demonstrates the amount of uncollected medical waste in the hospitals. It is clear that for example, 115 kg of medical waste has not been collected in Hospital 1.
7.3 Sensitivity analysis
In this subsection, main parameters of the proposed model are analyzed. Therefore, Fig. 18 demonstrates the relevance between the duration of fever, headache, and body aches. It also shows how people with these symptoms are assigned to different types of membership functions. It is clear that if the duration of fever and headache is zero, people are healthy (type 1). The longer the fever and headache last, the more the membership function moves to type 5.

Relationship between fever and tiredness
Figure 19 shows the changes in the number of established detoxification centers in terms of changes in amount of waste generated by hospitals. As it is known, with the increase of amount of waste generated by hospitals, more centers have been established. With a 30% reduction in amount of waste generated by hospitals, three detoxification centers have been established. This is if 10 centers have been established with an increase in amount of waste of up to 30%. The reason for the constant number of established centers in the 20 and 30% increase in amount of waste is the limited number of established centers.

The sensitivity analysis of the established detoxification centers based on changes in demands
Figure 20 displays the rate of change of the Environmental effect in terms of changes in amount of waste generated by hospitals. As it is known, with the increase of the changes in amount of waste generated by hospitals, environmental effect will also increase. For example, with a 30% decrease in changes in amount of waste generated by hospitals, the amount of environmental effect decreases to 32,057, and with a 30% increase in amount of waste generated by hospitals, the environmental effect increases to 99,412. Also, with a 20% increase in amount of waste generated by hospitals, the environmental effect increases to 79,111, and with a 20% decrease in amount of waste generated by hospitals, the environmental effect decreases to 41,670.

The sensitivity analysis of the environmental effect based on amount of waste generated
8 Conclusion and future works
In this paper, a new sustainable COVID-19 medical waste supply chain network for location and allocation decisions considering detoxification centers and waste management has been developed. Additionally, an MILP model has been formulated to the total costs, social responsibility, and environmental effects. Then, an FIS to forecast the COVID-19 medical wastes has been suggested. Then, people have been divided into four groups containing healthy people, suspicious, suspected of mild COVID-19, and suspicious. In the mathematical model, disposal centers, potential location for temporary detoxification centers, and existing detoxification centers simultaneously are considered for the first time. In addition, the location and distribution decisions of the COVID-19 medical wastes simultaneous are determined. Accordingly, a new heuristic method based on the artificial intelligence methods namely GOA and TS algorithms called modified Grasshopper Optimization Algorithm and Tabu Search (MGOTSA) has been developed for the first time in this paper to solve the presented model. Also, the GOA algorithm gets stuck in local optima, based on the poor exploitation and exploration. In the current work, a neighbor method from the TS algorithm is incorporated for the attained the best solution from the main loop of the GOA in each iteration to modify the efficiency of GOA. The Taguchi method has been utilized to tune and control the algorithm’s parameters. Then, to show the efficiency of the proposed algorithms, algorithms have been compared based on CPU time and assessment metrics. As a result, the MGOTSA algorithm had high quality and convergence than the TS and GOA algorithms as well as had low CPU. The results indicate that temporary detoxification centers 2, 7, and 10 are not established. Also, the results of sensitivity analysis show that, the longer the fever and headache last, the more the membership function moves to type 5. As demand increases, the number of established detoxification center increases. For instance, a 30% increase in demand will lead to the establishment of 10 detoxification center. Finally, as the amount of waste generated increases, the environmental effect increases. Eventually, a real case study in Tehran/Iran during the COVID-19 condition has been suggested to validate the developed model. The results of the FIS indicate that the decision-makers should utilize an FIS to forecast the COVID-19 medical waste.
There are several research directions that can be further followed according to this study. The proposed model in this study can be extended with sustainability, resiliency, and efficiency concepts. In addition, some resiliency measures can be used in order to enhance the efficiency of the suggested model. Other objective functions can be studied in the model, such as transportation risk minimization. Also, uncertainty methods such as fuzzy, robust, stochastic, and so on can be utilized to cope with uncertain parameters. We can recommend that the interested researchers add treatment, recycling, and disposal centers to the presented network. In terms of the solution methods, other approaches such as exact methods (benders decomposition, Lagrangian relaxation, etc.) and other meta-heuristics can be used to solve the proposed model. Finally, Internet-of-Things concepts can be added to the proposed model.
References
Ahmad, F., Ahmad, S., & Zaindin, M. (2021). Sustainable production and waste management policies for COVID-19 medical equipment under uncertainty: a case study analysis. Computers & Industrial Engineering, 157, 107381.
Alkahtani, M., Omair, M., Khalid, Q. S., Hussain, G., Ahmad, I., & Pruncu, C. (2021). A covid-19 supply chain management strategy based on variable production under uncertain environment conditions. International Journal of Environmental Research and Public Health, 18(4), 1662.
Behnood, A., Golafshani, E. M., & Hosseini, S. M. (2020). Determinants of the infection rate of the COVID-19 in the US using ANFIS and virus optimization algorithm (VOA). Chaos, Solitons & Fractals, 139, 110051.
Castillo, O., Castro, J. R., Pulido, M., & Melin, P. (2022). Interval type-3 fuzzy aggregators for ensembles of neural networks in COVID-19 time series prediction. Engineering Applications of Artificial Intelligence, 114, 105110.
Chou, X., Gambardella, L. M., & Montemanni, R. (2021). A Tabu Search algorithm for the Probabilistic Orienteering Problem. Computers & Operations Research, 126, 105107.
Dinh, P. H. (2021). A novel approach based on grasshopper optimization algorithm for medical image fusion. Expert Systems with Applications, 171, 114576.
Foy, B. H., Wahl, B., Mehta, K., Shet, A., Menon, G. I., & Britto, C. (2021). Comparing COVID-19 vaccine allocation strategies in India: A mathematical modelling study. International Journal of Infectious Diseases, 103, 431–438.
Glover, F. (1986). Future paths for integer programming and links to artificial intelligence. Computers & Operations Research, 13(5), 533–549.
Goodarzian, F., Ghasemi, P., Gunasekaren, A., Taleizadeh, A. A., & Abraham, A. (2021b). A sustainable-resilience healthcare network for handling COVID-19 pandemic. Annals of operations research, 1–65.
Goodarzian, F., Taleizadeh, A. A., Ghasemi, P., & Abraham, A. (2021b). An integrated sustainable medical supply chain network during COVID-19. Engineering Applications of Artificial Intelligence, 100, 104188.
Karmaker, C. L., Ahmed, T., Ahmed, S., Ali, S. M., Moktadir, M. A., & Kabir, G. (2021). Improving supply chain sustainability in the context of COVID-19 pandemic in an emerging economy: Exploring drivers using an integrated model. Sustainable Production and Consumption, 26, 411–427.
Ly, K. T. (2020). A COVID-19 forecasting system using adaptive neuro-fuzzy inference. Finance Research Letters, 41, 101844.
Maleki, M., Mahmoudi, M. R., Heydari, M. H., & Pho, K. H. (2020). Modeling and forecasting the spread and death rate of coronavirus (COVID-19) in the world using time series models. Chaos, Solitons & Fractals, 140, 110151.
Melin, P., Sánchez, D., Monica, J. C., & Castillo, O. (2021). Optimization using the firefly algorithm of ensemble neural networks with type-2 fuzzy integration for COVID-19 time series prediction. Soft Computing, 1–38.
Melin, P., Sánchez, D., Castro, J. R., & Castillo, O. (2022). Design of Type-3 fuzzy systems and ensemble neural networks for COVID-19 time series prediction using a firefly algorithm. Axioms, 11(8), 410.
Mishra, A. R., Rani, P., Krishankumar, R., Ravichandran, K. S., & Kar, S. (2021). An extended fuzzy decision-making framework using hesitant fuzzy sets for the drug selection to treat the mild symptoms of Coronavirus Disease 2019 (COVID-19). Applied Soft Computing, 103, 107155.
Nikolopoulos, K., Punia, S., Schäfers, A., Tsinopoulos, C., & Vasilakis, C. (2021). Forecasting and planning during a pandemic: COVID-19 growth rates, supply chain disruptions, and governmental decisions. European Journal of Operational Research, 290(1), 99–115.
Saremi, S., Mirjalili, S., & Lewis, A. (2017). Grasshopper optimisation algorithm: Theory and application. Advances in Engineering Software, 105, 30–47.
Sarkar, K., Khajanchi, S., & Nieto, J. J. (2020). Modeling and forecasting the COVID-19 pandemic in India. Chaos, Solitons & Fractals, 139, 110049.
Shaban, W. M., Rabie, A. H., Saleh, A. I., & Abo-Elsoud, M. A. (2021). Detecting COVID-19 patients based on fuzzy inference engine and Deep Neural Network. Applied Soft Computing, 99, 106906.
Shadkam, E. (2021). Cuckoo optimization algorithm in reverse logistics: A network design for COVID-19 waste management. Waste Management & Research, 0734242X211003947.
Sharma, H. B., Vanapalli, K. R., Cheela, V. S., Ranjan, V. P., Jaglan, A. K., Dubey, B., & Bhattacharya, J. (2020). Challenges, opportunities, and innovations for effective solid waste management during and post COVID-19 pandemic. Resources, Conservation and Recycling, 162, 105052.
Si, A., Das, S., & Kar, S. (2021). Picture fuzzy set-based decision-making approach using Dempster-Shafer theory of evidence and grey relation analysis and its application in COVID-19 medicine selection. Soft Computing., 27(6), 3327–3341.
Tavana, M., Govindan, K., Nasr, A. K., Heidary, M. S., & Mina, H. (2021). A mathematical programming approach for equitable COVID-19 vaccine distribution in developing countries. Annals of Operations Research, 1–34.
Towell, G. G., & Shavlik, J. W. (1994). Knowledge-based artificial neural networks. Artificial Intelligence, 70(1–2), 119–165.
Acknowledgements
“This work was partially supported by the FWF Austrian Science Fund (Peiman Ghasemi): I 5908-G.”
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Goodarzian, F., Ghasemi, P., Gunasekaran, A. et al. A fuzzy sustainable model for COVID-19 medical waste supply chain network. Fuzzy Optim Decis Making 23, 93–127 (2024). https://doi.org/10.1007/s10700-023-09412-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10700-023-09412-8