
Abstract
Sex under the influence of psychoactive substances (SUIPS) has gained much attention in the press and scientific literature over the last years, especially among men who have sex with men (MSM). Concerns have thus far been expressed in relation to short-term physical health risks, like contracting bloodborne diseases, like viruses. However, much less is known about long-term mental health consequences of SUIPS, like depression, anxiety, and substance use disorders (SUD). Therefore, we systematically reviewed literature for evidence on mental health complications of SUIPS in MSM. SUIPS was associated with a lower general mental health status, and higher rates of depression, anxiety disorders and suicide ideation in 15 studies, and higher rates of SUD were found among MSM practicing SUIPS in four studies. Motives of SUIPS were increasing sexual performance, fear of rejection, anxiety, and low self-esteem among others. Furthermore, long-term mental health risks, as associated with some of the most frequently reported psychoactive substances in the context of SUIPS, include psychosis and substance dependence. Therefore, the present findings indicate that SUIPS is associated with mental disorders and that they are probably closely intertwined with motives for SUIPS and the long-term effects of using psychoactive substances. This underlines the need to address the presence of mental disorders in people practicing SUIPS, alongside the physical risks.
Similar content being viewed by others


Introduction
Sex under the influence of psychoactive substances (SUIPS) is the practice of taking (several) psychoactive substances either before or during sexual intercourse to increase the duration and intensity of sexual experiences and is most prevalent among men having sex with men (MSM) (Edmundson et al., 2018; Maxwell et al., 2019). In Western Europe, this practice is often termed “chemsex.” SUIPS is worrisome because of its risk of adverse physical health effects: alongside the increased risk of dangerous intoxications, it increases the risk of sexually transmitted infections (STIs), like infections with the human immunodeficiency virus (HIV) and the hepatitis C virus (HCV) (Hegazi et al., 2017; Ireland et al., 2017; Maxwell et al., 2019). SUIPS is associated with taking risks, including condomless anal sex and prolonged sexual intercourse with different partners (Ahmed et al., 2016; Hegazi et al., 2017; Knoops et al., 2022; Maxwell et al., 2019; Pufall et al., 2018), and risky drug use behaviors, including intravenous drug injection, sometimes referred to as “slamming” or “slamsex” (Daskalopoulou et al., 2014, 2017; Dolengevich-Segal et al., 2019; Heinsbroek et al., 2018; Knoops et al., 2022; Melendez-Torres et al., 2018), together resulting in a high risk of (bloodborne) STIs. Actually, there is an increased incidence of these bloodborne diseases, which was partly attributed to the rise of SUIPS (Hagan et al., 2015; Vaux et al., 2019).
The first studies that raised concern about the practice of SUIPS among MSM were from the USA, mainly in the greater metropolitan areas, and largely involving the use of methamphetamine or “crystal meth” before or during sexual intercourse (Braine et al., 2011; Grov et al., 2014; Lyons et al., 2010; Mattison et al., 2001; Nanín et al., 2006). This was followed by many reports on the same phenomenon from Western Europe, where the term “chemsex” was introduced for SUIPS among MSM, with most studies investigating the risk of bloodborne STIs in gay communities in larger metropolitan areas within the UK (Ahmed et al., 2016; Bourne et al., 2015; Curtis et al., 2020; Edmundson et al., 2018; Hegazi et al., 2017; Hibbert et al., 2019; Kohli, et al., 2019; Macgregor et al., 2021; Melendez-Torres et al., 2018; Sewell et al., 2017; Tomkins et al., 2018; Weatherburn et al., 2017). More recently, several other European countries, including the Netherlands (Achterbergh et al., 2020; Drückler et al., 2018), Germany (Deimel et al., 2016), Belgium (Kenyon et al., 2018), Sweden (Dennermalm et al., 2021), Spain (González-Baeza et al., 2018), Ireland (Glynn et al., 2018), France (Vaux et al., 2019), and Italy (Latini et al., 2019), have also reported SUIPS among MSM and its association with STIs, like HIV, HCV, gonorrhea, and syphilis. In addition, SUIPS among MSM has been reported in Canada (Flores Anato et al., 2021), Australia (Hammoud et al., 2018), China (Wang et al., 2020; Wong et al., 2020), Vietnam (Vu et al., 2017), and Brazil (Torres et al., 2020), indicating that it is a worldwide phenomenon.
In a US national probability sample describing the prevalence of psychoactive substance use, sexual minorities (gay and bisexual men and women) reported a 2 to 4 times higher incidence of SUIPS than in heterosexual men and women (Rosner et al., 2021). However, most figures about the prevalence of SUIPS are only available for specific subgroups (EMCDDA, 2017). A survey from the UK among 3933 MSM showed that in the last year, 10% of MSM engaged in SUIPS (Blomquist et al., 2020), and another study among 2328 MSM from Scotland, Wales, Northern Ireland, and Ireland reported a last year prevalence of 8% (Frankis et al., 2018). In Hongkong (n = 407) (Wang et al., 2020), Germany (n = 1583) (Schecke et al., 2019), and across multiple European cities (n = 1261) (Rosińska et al., 2018), last year prevalence of SUIPS among MSM was 6.6%, 27%, and 11.8%, respectively. Higher rates are found (> 20%) in specific subgroups of MSM, like HIV-positive MSM at sexual health clinics (Bohn et al., 2020; Donnadieu-Rigole et al., 2020; Sewell et al., 2017).
Most studies report that MSM practicing SUIPS are generally well educated and employed with well-paid jobs (Deimel et al., 2016; Graf et al., 2018; Knoops et al., 2022; Mattison et al., 2001; Schecke et al., 2019). Research generally reports MSM practicing SUIPS as between 25 and 45 years (Blomquist et al., 2020; Graf et al., 2018; Guerras et al., 2020; Schecke et al., 2019; Schmidt et al., 2016). One out of four MSM used more than one psychoactive substance just before or during sex, and, thus, polydrug use seems to be quite common (Rosińska et al., 2018). Whereas most research focusses on MSM, SUIPS was also reported in lesbian and bisexual women, and often at a considerably higher prevalence than in heterosexual people (Lawn et al., 2019; Rosner et al., 2021). In fact, one study on heterosexual men and women at sexual health clinics and HIV-outpatient clinics did not find any SUIPS (Miltz et al., 2021).
Motives for Engaging in SUIPS
Various studies have tried to elucidate motives for SUIPS, such as increased libido, stamina, confidence, and disinhibition, as well as increased pleasure, attractiveness of sexual partners, intimacy, intense sensations, and sexual adventure (González-Baeza et al., 2018; Graf et al., 2018; Weatherburn et al., 2017). Participants of a German qualitative study also reported the realization of particular sexual fantasies (e.g. better sex, more sexual partners) as an important motive for SUIPS (Graf et al., 2018). Fear of rejection by sexual partners and coping with societal rejection, loneliness, anxiety, and low self-esteem were mentioned in two qualitative studies from Singapore (Tan et al., 2018, 2021), with HIV-related stigma, racism, sexual violence, and internalized homophobia as the main drivers of these motives (Tan et al., 2021). Finally, an Italian study found that some MSM practice SUIPS to cope with stress, depression, and anxiety symptoms, including sexual performance anxiety (Nimbi et al., 2021).
Theoretical Models Underlying SUIPS
During the second European Chemsex Forum in Berlin in 2018, people who engage in SUIPS (“chemsex”), community organizers, researchers, clinicians, therapists, social workers, and (peer) counselors discussed potential pathways to problematic SUIPS, and the findings of this meeting were then translated into a theoretical framework called the “Journey towards problematic chemsex use” (Platteau et al., 2019). In this framework, childhood adversities, feelings of loneliness, and emptiness may result in a search for interpersonal and sexual connectedness and finally SUIPS or “chemsex.” In addition, some of the users may lose their grip on other aspects of life (e.g., work responsibilities, finances, friendships, and family relationships), and ultimately, this loss of control over their life can lead to feelings of helplessness, depression, anxiety, and/or substance use disorders. For a schematic overview, see supplemental Fig. 1.
In addition to this specific pathway between SUIPs and mental health problems, there are at least two other pathways that may cause increased prevalences of mental disorders in MSM that engage in SUIPS: minority stress theory and syndemic theory. Minority stress theory describes the psychosocial consequences of being in continual conflict with a discriminatory and heteronormative social environment. Perpetual negative feedback from others is thought to lead to a process of self-stigmatization termed internalized homophobia, whereby antigay social values/attitudes are directed towards the self. Internalized homophobia often results in deep conflict and poor self-regard with negative consequences such as pervasive expectations of rejection in one’s life and concealment of one’s sexual identity. Concealment adds to mental distress by disallowing individuals to affiliate with people of the same sexual identity (Meyer, 2003; Miltz et al., 2019). Syndemic mechanisms involve the synergistic interaction of risk factors such as concomitant use of recreational drugs and the experiences of intimate partner violence among sexual minorities that are associated with mental health problems due to causal and bidirectional relationships between these and other risk factors (Miltz et al., 2019). Based on these different—but overlapping and interacting—personal and social processes, we expect high levels of mental problems in people who engage in SUIPS.
Substances Involved in SUIPS: Definition
SUIPS substances, used shortly before or during sexual intercourse, are often distinct from those that are used during a regular night out (e.g., club, venue, and bar), like alcohol, cannabis, and tobacco (Drückler et al., 2018; Frankis et al., 2018; Hegazi et al., 2017; Melendez-Torres et al., 2018; Pakianathan et al., 2016; Weatherburn et al., 2017). In a UK study, methamphetamine (crystal meth), gamma hydroxybutyric acid/gamma butyrolactone (GHB/GBL), and synthetic cathinones (e.g., mephedrone) were reported as typical SUIPS substances (Bourne et al., 2015). Together with ketamine, these substances were also reported in a large European internet survey in 44 major cities across Europe. Crystal meth, GHB/GBL, mephedrone, and ketamine were also reported in Germany and The Netherlands as the most frequently used SUIPS substances (Achterbergh et al., 2020; Evers et al., 2020; Schecke et al., 2019). Finally, all these substances were also detected by toxicological analysis of the nails of individuals practicing SUIPS in Italy (Busardò et al., 2020).
Although a clear definition of SUIPS substances is lacking, the prevalence of the most frequently reported psychoactive substances in 255 initial screened articles is shown in Fig. 1. For the sake of comparison, the prevalence of cannabis (as not typically associated with SUIPS) is also depicted in Fig. 1, as many studies asked out a generic list of substances. These data show the high prevalence of methamphetamine/crystal meth, GHB/GBL, ketamine, and synthetic cathinones (e.g., mephedrone) in SUIPS among MSM (e.g., Bohn et al., 2020; Bourne et al., 2015; Evers et al., 2019; Maxwell et al., 2019; Schmidt et al., 2016; Wang et al., 2023). Poppers and erectile dysfunction drugs (EDs) were also reported to be frequently used before and during sex by MSM but are not seen as psychoactive substance, since they do not target the brain. Also, EDs and poppers are used in a more generic and casual way than the psychoactive substances involved in a SUIPS or “chemsex” session.

Substances reported most frequently in scientific literature about sex under the influence of psychoactive substances among MSM
Aim of This Review
Summarizing, our knowledge on SUIPS among MSM has been growing vastly throughout the years, but most of it has been focussed on the short-term physical risks, i.e., intoxications and STIs. Less well described are long-term mental health consequences of SUIPS in MSM. Our hypothesis is that SUIPS is associated with an increase in mental health problems, based on the nature of the psychoactive substances involved, motives, and the theoretical models described above. The main objective of this review is, therefore, to systematically synthesize the scientific literature on the long-term mental health complications of SUIPS among MSM, like depression, anxiety, or substance use disorders (SUD). The causal interpretation of our findings regarding the relationships between SUIPS and mental health problems is then discussed.
Methods
Eligibility
For our review on the mental health and SUIPS, the Preferred Reporting Items for Systematic Reviews and Meta Analyses protocol (PRISMA) was used (Liberati et al., 2009). The following criteria were used for eligibility: (1) published in English from 1 January 2001 to 1 April 2023; (2) cross-sectional study, longitudinal study, cohort study, and case–control study; (3) standardized instruments to assess mental disorders, including depression, anxiety, and SUD; (4) statistical outcomes; (5) population of MSM aged 18 and above; (6) psychoactive substances used just before or during sexual intercourse, excluding alcohol and/or tobacco as the only substances.
Poppers and erectile dysfunction drugs (EDs) are not deemed as typical of SUIPS since they do not belong to the group of psychoactive substances and do not typically target the brain, and studies were therefore excluded as well, if they were the only substances mentioned. In that sense, among other things, our review differs from a previously published review about mental health symptoms and sexualized drug use in MSM, which included poppers, EDs, and even cannabis as the only drugs mentioned (Íncera-Fernández et al., 2021). Not only are these drugs not regarded as typical for SUIPS or “chemsex,” our hypothesis anticipates negative effects as a result of using substances that actually target the brain and are thus related to mental health issues.
The following paper types were excluded: review papers, conference abstracts, case reports, and exclusively qualitative studies, protocol descriptions without study data.
Databases
Two authors (TB, NG) independently searched five databases: (1) PsycINFO; (2) PubMed; (3) EBSCO, (4) CINAHL, and (5) SCOPUS.
Search Terms
The following search terms were used: Sex under influence OR sex under influence of psychoactive substances OR chemsex OR sex drugs OR sex illicit drug use OR slamming OR slamsex AND men who have sex with men OR MSM OR gay or homosexual OR bisexual AND mental health OR mental well-being OR psychopathology OR disorder OR dependence OR addiction OR depression OR anxiety OR substance use disorder OR withdrawal OR craving OR substance abuse.
Study Selection
Scientific papers were screened in two stages: (1) title/abstract screening and (2) full-text screening. Titles and abstracts were then filtered using the eligibility criteria. Full texts were assembled for eligible articles. These were reviewed by two authors (TB, NG) for inclusion criteria independently, and a third author (DD) acted as a tie-breaker when there was no consensus reached between the initial two authors.
Data Compilation
The following characteristics of the screened papers were compiled into a large table: first author, year, timing of data collection, study design, psychometric instruments used, study location, sample size, sample characteristics, and main study outcomes/conclusions (Table 1).
Quality Assessment and Outcome Robustness
Two authors (TB, NG) assessed the quality of the eligible studies using the Joanna Briggs Institute (JBI) Appraisal Tools for cross-sectional and cohort studies. Based on these appraisal tools, it was decided to include or to exclude studies. This was discussed among both assessors, and when they disagreed, a third author was consulted. It was decided that only significant (p < 0.05) differences between study groups were included as outcomes.
Results
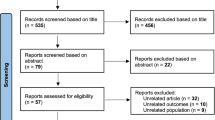
In total, 394 articles were identified via the electronic databases, and after removing duplicates, this was reduced to 255. Then, 211 articles were excluded after screening abstracts for case reports, reviews, non-English written, and non-mental health-related (for instance, only STI-related) outcomes, leaving 44 articles. After careful evaluation of these 44 articles, 25 additional articles were excluded (e.g., case series, no statistical outcomes). Figure 2 shows the PRISMA flowchart of the selection procedure.

Schematic presentation of the PRISMA study selection procedure
Table 1 summarizes the studies collected in this systematic review, describing mental health outcomes associated with SUIPS (sex under influence of psychoactive substances). A total of 19 studies were selected for evaluation, including 18 cross-sectional studies and one longitudinal study with a focus on MSM recruited either through targeted social media platforms (Hibbert et al., 2019; Li et al., 2021; Tan et al., 2021; Torres et al., 2020) or via sexual health clinics counseling MSM for STI, HIV-status, and the use of (post exposure or pre-exposure) prophylaxis (Hampel et al., 2020; Sewell et al., 2017). In the following paragraphs, associations between the mental health and SUIPS are described.
General Mental Health
Several MSM studies report that MSM do not experience adverse effects of SUIPS (Drückler et al., 2018; Evers et al., 2020; Graf et al., 2018) and neither do they perceive the need to change their SUIPS behavior (Evers et al., 2020; Lafortune et al., 2021; Lea et al., 2019). However, three studies reported the presence of an impaired general, not clinically specified, mental health status in SUIPS users (Table 1). In a large cross-sectional study (n = 2,610) among MSM in five major French cities, it was found that the general mental health status of MSM practicing injecting drug use before and during sexual intercourse (“slamsex”) in the last year was 10% lower than MSM who had never practiced it (Trouiller et al., 2020). A large web survey (n = 1648) from the UK found lower life satisfaction in MSM practicing SUIPS in the last year compared to those that did not (Hibbert et al., 2019). Finally, in a Taiwanese study (n = 517), methamphetamine dependency as a result of SUIPS was accompanied by increased feelings of loneliness (Li et al., 2021).
Specified Mental Health Problems
In addition to the rather broad definitions of mental health used in the studies mentioned above, several other studies looked at the presence of specific types of psychopathology, mainly depression and anxiety. Eleven studies reported a significant positive association between SUIPS and depression, anxiety, and suicidal ideation among MSM, whereas two studies found no association, and one study even found a negative association (Table 1).
So, nine studies did establish a positive association between SUIPS and depression/anxiety in MSM. In a large cross-sectional study from England among 1484 HIV-negative or HIV-undiagnosed MSM from 20 sexual health clinics, SUIPS during the last 3 months before the study was associated with more symptoms of depression compared to those who did not engage in SUIPS (Sewell et al., 2017). In another study from the UK, among 392 MSM, those practicing SUIPS in the 12 months preceding the study were significantly more likely to self-report depression and anxiety than those not practicing SUIPS (Pufall et al., 2018). An Australian study among 3017 gay and bisexual men investigated both substance dependence and other psychopathological consequences of SUIPS and found an association between dependent methamphetamine use with depression and anxiety (Prestage et al., 2018). Among 357 German MSM, SUIPS was associated with slightly higher scores of anxiety, depression, and somatization (Bohn et al., 2020). The effect was strongest among those MSM using methamphetamine for its association with major depression (Schecke et al., 2019).
A large Swiss cohort study of people living with HIV found a substantial increase in the use of SUIPS drugs among 5657 MSM over 11 years (8.8% in 2007 vs. 13.8% in 2017) (Hampel et al., 2020). This increase mainly involved the use of methamphetamine, GHB/GBL, ketamine, and mephedrone, and the use of these substances over time was significantly associated with self-reported depression compared to non-use of those substances, although causality could not be established in this study. In a Spanish study among 742 MSM, injecting drug use during sex (i.e., “slamsex”) (n = 34) was more strongly associated with withdrawal, craving, and dependence than non-injecting SUIPS, and having these SUD symptoms was closely associated with depression severity, but not in the non-injecting SUIPS group (Dolengevich-Segal et al., 2019). Finally, in a Norwegian study among 1013 MSM visiting a STI clinic, both univariate and multivariate analyses identified SUIPS over the year preceding the study as a (statistical) predictor for psychopathology, particularly depression and anxiety (Berg et al., 2020).
In the study by Dolengevich-Segal et al. (2019), higher levels of psychotic symptoms and suicide ideation during or after sexual intercourse were also found in the injecting SUIPS group compared to the non-injecting SUIPS group. Elevated rates of suicidal ideation among MSM practicing SUIPS versus MSM not practicing SUIPS were also found in another study, together with higher depression severity (Tan et al., 2021). A German latent class analysis (LCA) found suicidal ideation and depressive mood among one-third of MSM using typical “chemsex” substances compared to MSM using poppers or alcohol (Scholz-Hehn et al., 2022). Finally, suicide ideation was reported among UK MSM practicing SUIPS, mainly in those using GHB (Stevens et al., 2020).
In contrast to these findings, one of the first studies (n = 214) about SUIPS in MSM and psychopathology failed to find an association between depression and SUIPS in the 12 months preceding the study (Mimiaga et al., 2008). A recent study from Norway (n = 518) also found no association between SUIPS in the last year preceding the study and self-reported depression/anxiety (Amundsen et al., 2022). Finally, a recent study among Dutch MSM living with HIV (n = 359) found no association between SUIPS and anxiety and even decreased odds of depression, but the authors noted that causality could not be inferred (Field et al., 2023).
Substance Use Disorders (SUD)
Surprisingly, given the frequent use of potentially addictive substances involved in SUIPS (Achterbergh et al., 2020; Schmidt et al., 2016; Van Hout et al., 2019), few studies have investigated the prevalence of SUD in people practicing SUIPS. We found four studies, all reporting statistically significantly more SUD in MSM practicing SUIPS compared to MSM not practicing SUIPS (Table 1).
A Brazilian study of 1048 MSM looked at the risk for SUD with the WHO Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) and found that MSM practicing SUIPS in the 3 months before the study were much more likely to have a high SUD risk than MSM not practicing it: 64% vs. 17.5%, respectively (Torres et al., 2020). In a recent study in Taiwan, nearly half of all 517 MSM practicing SUIPS showed methamphetamine dependency according to the severity of dependence scale (SDS) (Li et al., 2021). A Spanish study among 742 MSM specifically looked at slamsex vs. non-injecting SUIPS and found that the former group experienced more severe drug-related symptoms (withdrawal, craving, and dependence) and more symptoms of severe intoxication (Dolengevich-Segal et al., 2019). Unfortunately, no comparison was made with non-SUIPS practicing MSM. Finally, in a small sample of 34 French cathinone-injecting slamsex users, 33 met the criteria for SUD according to DSM-5 (Schreck et al., 2020). Out of these, 19 (56%) met the criteria for severe SUD and were identified as “cathinone use disorder,” although most were polydrug users.
Discussion
SUIPS (also referred to as “chemsex”) is a worldwide sexual practice of men having sex with men (MSM), which seems to be increasing. SUIPS involves potentially addictive substances which are often administered in hazardous manners (e.g., injecting) increasing the risks of STIs and substance use disorders (SUD). In fact, several studies have shown an increased risk for SUD among MSM practicing SUIPS compared to MSM who do not. In SUIPS, SUD seems particularly associated with the use of methamphetamine, synthetic cathinones, and GHB/GBL. In addition, SUIPS is also associated with higher rates of anxiety, (severity of) depression, and suicide ideation, whereas injecting drug use during sex (“slamsex”) might be associated with psychosis. Combined with the findings of general decreased mental health and lowered satisfaction with life among MSM engaging in SUIPS suggests an increased risk of long-term negative mental health consequences of this practice, confirming our hypothesis.
It is important to emphasize that six of the largest studies (> 1,000 participants), implicating greater statistical power, all confirmed psychopathological outcomes of SUIPS with validated psychometric instruments (Berg et al., 2020; Hampel et al., 2020; Prestage et al., 2018; Sewell et al., 2017; Torres et al., 2020; Trouiller et al., 2020). However, this review also retrieved three studies which did not find evidence for the negative mental health effects of SUIPS. The negative studies were similar to the positive studies in that they were all cross-sectional in nature, and they used validated instruments to assess depression and anxiety. However, all three negative studies had (relatively) small samples. We, therefore, conclude that the results of this review imply the need for health care professionals to look beyond the scope of the physical risks of SUIPS (like increased risks of STIs) and also consider the mental health status of MSM practicing SUIPS.
SUIPS appears to be a complex behavior with different motivations and objectives. Motives for SUIPS, like fear of rejection, loneliness, internalized homophobia, anxiety, and low self-esteem (Tan et al., 2018, 2021), may be underlying comorbidity with depression and/or anxiety, indicating that depression and anxiety can be both a cause and a consequence of SUIPS. Furthermore, the fact that HIV-positive MSM are overrepresented among MSM engaging in SUIPS may partly explain the increased risk of negative mental health problems since a HIV-positive status is associated with more symptoms of depression and anxiety (Remien et al., 2019). Comorbid methamphetamine and alcohol use disorders (not related to sex) in MSM (n = 286) were also associated with the presence of other mental disorders (e.g., social phobia, depression, and obsessive–compulsive), but no causality could be ascertained (Fletcher et al., 2018). Another study found that recent polydrug use (not related to sex) and depressive symptoms both mediated high-risk sexual behavior and HIV in MSM (Card et al., 2018). This may imply that both recent polydrug use and depression are factors underlying SUIPS. Therefore, the question whether SUIPS causes mental health problems or vice versa is still unanswered.
It seems that to practice SUIPS (“chemsex”) is rather specific for MSM and, to a lesser extent, the gay community as a whole, since the incidence of SUIPS—although relatively low in the gay community—was 2 to 4 times higher than in heterosexual men and women (Rosner et al., 2021). In fact, another study also showed that lesbian and bisexual women practiced SUIPS and that they did so at a substantial higher rate than heterosexual men or women (Lawn et al., 2019). The practice of SUIPS is more specific for sexual minorities and this was also demonstrated by a study in which heterosexual men and women visiting sexual health clinics and HIV-outpatient clinics were not reporting SUIPS (Miltz et al., 2021).
The psychoactive substances involved in SUIPS are all known to have (substantial) risks, either acute risks (psychosis, respiratory depression, and coma) or long-term risks (dependence, cognitive impairment). For instance, methamphetamine is a stimulant with a high addiction potential (Baicy & London, 2007; Barr et al., 2006), and frequent use can lead to severe cortical dysregulation and neuronal damage, resulting in impaired cognitive functioning (Baicy & London, 2007; Gold et al., 2009). Methamphetamine use is also associated with an increased prevalence of psychopathology, such as depression, psychosis, and antisocial personality disorder (Fletcher et al., 2018; Glasner-Edwards & Mooney, 2014; Schecke et al., 2019). Like methamphetamine, synthetic cathinones are potent dopamine releasers, and their risks are similar (Donnadieu-Rigole et al., 2020; Karila et al., 2018). Furthermore, the anesthetic drugs ketamine and GHB/GBL show substantial dependence liability (Busardo & Jones, 2014; Gonzalez & Nutt, 2005; Liao et al., 2018), with excited delirium as a severe withdrawal symptom of GHB (Brunt et al., 2014; Kamal et al., 2017; Lingford-Hughes et al., 2016). GHB overdosing quickly results in nausea, respiratory depression, and coma (Karila & Reynaud, 2011). The risks of GHB/GBL use seem to be prominent in MSM communities (Corkery et al., 2018), e.g., the increase in GHB-induced fatalities was partly ascribed to the rise of SUIPS behavior in London (Hockenhull et al., 2017). Taking these well-known risks of substances involved in SUIPS into account, the reported increase of adverse mental health conditions does not come as a surprise.
Polydrug use is commonplace among MSM practicing SUIPS, and this further contributes to these risks, as combining several drugs may lead to unpredictable interaction effects, like the combination of alcohol and GHB, and these combinations may also complicate detoxification efforts (Morse & Morris, 2013). Since SUIPS is particularly prevalent in HIV-positive MSM, it is also worth mentioning that substances like methamphetamine and MDMA interact with antiretroviral drug treatment (Bracchi et al., 2015). Therefore, treatment professionals need to remain cautious of these adverse consequences when dealing with MSM practicing SUIPS and to be aware of long-term mental health problems, including SUD and depression/anxiety.
Apart from the types of psychoactive substances that are used in SUIPS, the route of administration was found to play an important role in the mental health impact of SUIPS: slamming (injecting drugs preceding and during sex) was associated with an increased risk for SUD and other mental disorders compared to non-injecting SUIPS (Dolengevich-Segal et al., 2019; Melendez-Torres et al., 2018; Trouiller et al., 2020). This seems especially true for methamphetamine and synthetic cathinones (Schreck et al., 2021).
There seems to be a need for mental health screening in MSM who frequently practice SUIPS because of the frequent mental health problems experienced in MSM practicing SUIPS (Evers et al., 2020). In a large, representative, national population survey from the USA (n = 8241), a perceived unmet need for psychological treatment was primarily reported by MSM practicing SUIPS compared to other groups of the population, including bi-/heterosexual people and MSM not practicing SUIPS (Rosner et al., 2021). This demand for psychological counseling in MSM practicing SUIPS was also reported in other studies (Arends et al., 2020; Parry et al., 2019) and represents an important implication that is underscored by this review.
Limitations
Although this review is based on a systematic search of the literature, it has limitations. First, because of the cross-sectional nature of most studies, it was not possible to ascertain a causal relationship between SUIPS and any of the mental disorders investigated. Mental health problems or polydrug use may underlie the propensity for engaging in SUIPS just as well as SUIPS may be the cause of mental health problems. Second, the self-report nature of the data in most studies limits the assumed validity of the observed associations, because participants may not correctly recall the substance(s) that were used at a sexual event, and self-reported measures of mental problems may overestimate the prevalence of clinically relevant mental disorders. Also, time points at which the substances were taken around and during the sexual event are in some studies inconclusive. Therefore, it is recommended for future research (a) to consolidate the substances used during SUIPS via drug testing (blood, urine, or saliva), (b) to use structured interviews that establish psychiatric diagnoses, (c) to use longitudinal/prospective designs, and (d) to include the history of mental health problems (including substance dependence) of the study participants.
Conclusion
SUIPS (“çhemsex”) is an emerging and worldwide health concern. The practice of SUIPS is inherently associated with several health risks which are mainly related to the type of sexual behaviors (e.g., unprotected anal sex), the (combinations of) substances that are used, and the route of administration of these substances (e.g., slamsex). SUIPS is not only associated with an increased risk for STIs but is also associated with an increased risk for mental disorders, including SUD, suicide ideation and depression/anxiety. Screening, counseling, and treatment strategies should, therefore, consider both domains (e.g., Achterbergh et al., 2021), especially as many MSM practicing SUIPS do express the need for psychological support.
References
Achterbergh, R. C. A., de Vries, H. J. C., Boyd, A., Davidovich, U., Drückler, S., Hoornenborg, E., Prins, M., & Matser, A. (2020). Identification and characterization of latent classes based on drug use among men who have sex with men at risk of sexually transmitted infections in Amsterdam, the Netherlands. Addiction, 115(1), 121–133. https://doi.org/10.1111/add.14774
Achterbergh, R. C. A., Van Rooijen, M. S., Van den Brink, W., Boyd, A., & De Vries, H. J. C. (2021). Enhancing help-seeking behaviour among men who have sex with men at risk for sexually transmitted infections: The syn.bas.in randomised controlled trial. Sexually Transmitted Infections, 97(1), 11–17. https://doi.org/10.1136/sextrans-2020-054438
Ahmed, A. K., Weatherburn, P., Reid, D., Hickson, F., Torres-Rueda, S., Steinberg, P., & Bourne, A. (2016). Social norms related to combining drugs and sex (“chemsex”) among gay men in South London. International Journal of Drug Policy, 38, 29–35. https://doi.org/10.1016/j.drugpo.2016.10.007
Amundsen, E., Haugstvedt, Å., Skogen, V., & Berg, R. C. (2022). Health characteristics associated with chemsex among men who have sex with men: Results from a cross-sectional clinic survey in Norway. PLoS One, 17(10). https://doi.org/10.1371/JOURNAL.PONE.0275618
Arends, R. M., van den Heuvel, T. J., Foeken-Verwoert, E. G. J., Grintjes, K. J. T., Keizer, H. J. G., Schene, A. H., van der Ven, A. J. A. M., & Schellekens, A. F. A. (2020). Sex, drugs, and impulse regulation: A perspective on reducing transmission risk behavior and improving mental health among MSM living with HIV. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.01005
Baicy, K., & London, E. D. (2007). Corticolimbic dysregulation and chronic methamphetamine abuse. In Addiction (Vol. 102, Issue SUPPL. 1, pp. 5–15). Addiction. https://doi.org/10.1111/j.1360-0443.2006.01777.x
Barr, A. M., Panenka, W. J., MacEwan, G. W., Thornton, A. E., Lang, D. J., Honer, W. G., & Lecomte, T. (2006). The need for speed: An update on methamphetamine addiction. In Journal of Psychiatry and Neuroscience (Vol. 31, Issue 5, pp. 301–313). Canadian Medical Association.
Berg, R. C., Amundsen, E., & Haugstvedt, Å. (2020). Links between chemsex and reduced mental health among Norwegian MSM and other men: Results from a cross-sectional clinic survey. BMC Public Health, 20(1). https://doi.org/10.1186/s12889-020-09916-7
Blomquist, P. B., Mohammed, H., Mikhail, A., Weatherburn, P., Reid, D., Wayal, S., Hughes, G., & Mercer, C. H. (2020). Characteristics and sexual health service use of MSM engaging in chemsex: Results from a large online survey in England. Sexually Transmitted Infections, 96(8), 590–595. https://doi.org/10.1136/sextrans-2019-054345
Bohn, A., Sander, D., Köhler, T., Hees, N., Oswald, F., Scherbaum, N., Deimel, D., & Schecke, H. (2020). Chemsex and mental health of men who have sex with men in Germany. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.542301
Bourne, A., Reid, D., Hickson, F., Torres-Rueda, S., Steinberg, P., & Weatherburn, P. (2015). “Chemsex” and harm reduction need among gay men in South London. International Journal of Drug Policy, 26(12), 1171–1176. https://doi.org/10.1016/j.drugpo.2015.07.013
Bracchi, M., Stuart, D., Castles, R., Khoo, S., Back, D., & Boffito, M. (2015). Increasing use of ‘party drugs’ in people living with HIV on antiretrovirals. AIDS, 29(13), 1585–1592. https://doi.org/10.1097/QAD.0000000000000786
Braine, N., Acker, C. J., Van Sluytman, L., Friedman, S., & Des Jarlais, D. C. (2011). Drug use, community action, and public health: Gay men and crystal meth in NYC. Substance Use & Misuse, 46(4), 368–380. https://doi.org/10.3109/10826081003720899
Brunt, T., Amsterdam, J., & Brink, W. (2014). GHB, GBL and 1,4-BD addiction. Current Pharmaceutical Design, 20(25), 4076–4085. https://doi.org/10.2174/13816128113199990624
Busardò, F. P., Gottardi, M., Pacifici, R., Varì, M. R., Tini, A., Volpe, A. R., Giorgetti, R., & Pichini, S. (2020). Nails analysis for drugs used in the context of chemsex: A pilot study. Journal of Analytical Toxicology, 44(1), 69. https://doi.org/10.1093/jat/bkz009
Busardo, F., & Jones, A. (2014). GHB pharmacology and toxicology: Acute intoxication, concentrations in blood and urine in forensic cases and treatment of the withdrawal syndrome. Current Neuropharmacology, 13(1), 47–70. https://doi.org/10.2174/1570159x13666141210215423
Card, K. G., Lachowsky, N. J., Armstrong, H. L., Cui, Z., Wang, L., Sereda, P., Jollimore, J., Patterson, T. L., Corneil, T., Hogg, R. S., Roth, E. A., & Moore, D. M. (2018). The additive effects of depressive symptoms and polysubstance use on HIV risk among gay, bisexual, and other men who have sex with men. Addictive Behaviors, 82, 158–165. https://doi.org/10.1016/j.addbeh.2018.03.005
Corkery, J. M., Loi, B., Claridge, H., Goodair, C., & Schifano, F. (2018). Deaths in the lesbian, gay, bisexual and transgender United Kingdom communities associated with GHB and precursors. Current Drug Metabolism, 19(13), 1086–1099. https://doi.org/10.2174/1389200218666171108163817
Curtis, T. J., Rodger, A. J., Burns, F., Nardone, A., Copas, A., & Wayal, S. (2020). Patterns of sexualised recreational drug use and its association with risk behaviours and sexual health outcomes in men who have sex with men in London, UK: A comparison of cross-sectional studies conducted in 2013 and 2016. Sexually Transmitted Infections, 96(3), 197–203. https://doi.org/10.1136/sextrans-2019-054139
Daskalopoulou, M., Rodger, A., Phillips, A. N., Sherr, L., Speakman, A., Collins, S., Elford, J., Johnson, M. A., Gilson, R., Fisher, M., Wilkins, E., Anderson, J., McDonnell, J., Edwards, S., Perry, N., O’Connell, R., Lascar, M., Jones, M., Johnson, A. M., …, & Lampe, F. C. (2014). Recreational drug use, polydrug use, and sexual behaviour in HIV-diagnosed men who have sex with men in the UK: Results from the cross-sectional ASTRA study. The Lancet HIV, 1(1), e22–e31. https://doi.org/10.1016/S2352-3018(14)70001-3
Daskalopoulou, M., Rodger, A. J., Phillips, A. N., Sherr, L., Elford, J., McDonnell, J., Edwards, S., Perry, N., Wilkins, E., Collins, S., Johnson, A. M., Burman, W. J., Speakman, A., & Lampe, F. C. (2017). Condomless sex in HIV-diagnosed men who have sex with men in the UK: Prevalence, correlates, and implications for HIV transmission. Sexually Transmitted Infections, 93(8), 590–598. https://doi.org/10.1136/sextrans-2016-053029
Deimel, D., Stöver, H., Hößelbarth, S., Dichtl, A., Graf, N., & Gebhardt, V. (2016). Drug use and health behaviour among German men who have sex with men: Results of a qualitative, multi-centre study. Harm Reduction Journal, 13(1). https://doi.org/10.1186/s12954-016-0125-y
Dennermalm, N., Scarlett, J., Thomsen, S., Persson, K. I., & Alvesson, H. M. (2021). Sex, drugs and techno – a qualitative study on finding the balance between risk, safety and pleasure among men who have sex with men engaging in recreational and sexualised drug use. BMC Public Health, 21(1). https://doi.org/10.1186/s12889-021-10906-6
Dolengevich-Segal, H., Gonzalez-Baeza, A., Valencia, J., Valencia-Ortega, E., Cabello, A., Tellez-Molina, M. J., Perez-Elias, M. J., Serrano, R., Perez-Latorre, L., Martin-Carbonero, L., Arponen, S., Sanz-Moreno, J., Fuente, S. D. la, Bisbal, O., Santos, I., Casado, J. L., Troya, J., Cervero-Jimenez, M., Nistal, S., …, & Ryan, P. (2019). Drug-related and psychopathological symptoms in HIV-positive men who have sex with men who inject drugs during sex (slamsex): Data from the U-SEX GESIda 9416 study. PLoS ONE, 14(12). https://doi.org/10.1371/journal.pone.0220272
Donnadieu-Rigole, H., Peyrière, H., Benyamina, A., & Karila, L. (2020). Complications related to sexualized drug use: What can we learn from literature? In Frontiers in Neuroscience (Vol. 14). Front Neurosci. https://doi.org/10.3389/fnins.2020.548704
Drückler, S., Van Rooijen, M. S., & De Vries, H. J. C. (2018). Chemsex among men who have sex with men: A sexualized drug use survey among clients of the sexually transmitted infection outpatient clinic and users of a gay dating app in Amsterdam, the Netherlands. Sexually Transmitted Diseases, 45(5), 325–331. https://doi.org/10.1097/OLQ.0000000000000753
Edmundson, C., Heinsbroek, E., Glass, R., Hope, V., Mohammed, H., White, M., & Desai, M. (2018). Sexualised drug use in the United Kingdom (UK): A review of the literature. International Journal of Drug Policy, 55, 131–148. https://doi.org/10.1016/j.drugpo.2018.02.002
EMCDDA. (2017). Drug-related infectious diseases in Europe. Retrieved 13-04-2023, from https://www.emcdda.europa.eu/system/files/publications/6462/20175424_TD0417745ENN_PDF.pdf
Evers, Y. J., Van Liere, G. A. F. S., Hoebe, C. J. P. A., & Dukers-Muijrers, N. H. T. M. (2019). Chemsex among men who have sex with men living outside major cities and associations with sexually transmitted infections: A cross-sectional study in the Netherlands. PLoS ONE, 14(5). https://doi.org/10.1371/journal.pone.0216732
Evers, Y. J., Hoebe, C. J. P. A., Dukers-Muijrers, N. H. T. M., Kampman, C. J. G., Kuizenga-Wessel, S., Shilue, D., Bakker, N. C. M., Schamp, S. M. A. A., Van Buel, H., Van Der Meijden, W. C. J. P. M., & Van Liere, G. A. F. S. (2020). Sexual, addiction and mental health care needs among men who have sex with men practicing chemsex – a cross-sectional study in the Netherlands. Preventive Medicine Reports, 18. https://doi.org/10.1016/j.pmedr.2020.101074
Field, D. J., de Wit, J., Davoren, M. P., O’Reilly, E. J., & Den Daas, C. (2023). Chemsex, anxiety and depression among gay, bisexual and other men who have sex with men living with HIV. AIDS and Behavior. https://doi.org/10.1007/S10461-023-04041-Z
Fletcher, J. B., Swendeman, D., & Reback, C. J. (2018). Mental health and substance use disorder comorbidity among methamphetamine-using men who have sex with men. Journal of Psychoactive Drugs, 50(3), 206–213. https://doi.org/10.1080/02791072.2018.1447173
Flores Anato, J. L., Panagiotoglou, D., Greenwald, Z. R., Trottier, C., Vaziri, M., Thomas, R., & Maheu-Giroux, M. (2021). Chemsex practices and pre-exposure prophylaxis (PrEP) trajectories among individuals consulting for PrEP at a large sexual health clinic in Montréal, Canada (2013–2020). Drug and Alcohol Dependence, 226. https://doi.org/10.1016/j.drugalcdep.2021.108875
Frankis, J., Flowers, P., McDaid, L., & Bourne, A. (2018). Low levels of chemsex among men who have sex with men, but high levels of risk among men who engage in chemsex: Analysis of a cross-sectional online survey across four countries. Sexual Health, 15(2), 144–150. https://doi.org/10.1071/SH17159
Glasner-Edwards, S., & Mooney, L. J. (2014). Methamphetamine psychosis: Epidemiology and management. CNS Drugs, 28(12), 1115–1126. https://doi.org/10.1007/s40263-014-0209-8
Glynn, R. W., Byrne, N., O’Dea, S., Shanley, A., Codd, M., Keenan, E., Ward, M., Igoe, D., & Clarke, S. (2018). Chemsex, risk behaviours and sexually transmitted infections among men who have sex with men in Dublin, Ireland. International Journal of Drug Policy, 52, 9–15. https://doi.org/10.1016/j.drugpo.2017.10.008
Gold, M. S., Kobeissy, F. H., Wang, K. K. W., Merlo, L. J., Bruijnzeel, A. W., Krasnova, I. N., & Cadet, J. L. (2009). Methamphetamine- and trauma-induced brain injuries: Comparative cellular and molecular neurobiological substrates. In Biological Psychiatry (Vol. 66, Issue 2, pp. 118–127). Biol Psychiatry. https://doi.org/10.1016/j.biopsych.2009.02.021
Gonzalez, A., & Nutt, D. J. (2005). Gamma hydroxy butyrate abuse and dependency. In Journal of Psychopharmacology (Vol. 19, Issue 2, pp. 195–204). J Psychopharmacol. https://doi.org/10.1177/0269881105049041
González-Baeza, A., Dolengevich-Segal, H., Pérez-Valero, I., Cabello, A., Téllez, M. J., Sanz, J., Pérez-Latorre, L., Bernardino, J. I., Troya, J., De La Fuente, S., Bisbal, O., Santos, I., Arponen, S., Hontañon, V., Casado, J. L., & Ryan, P. (2018). Sexualized drug use (chemsex) is associated with high-risk sexual behaviors and sexually transmitted infections in HIV-positive men who have sex with men: Data from the U-SEX GESIDA 9416 Study. AIDS Patient Care and STDs, 32(3), 112–118. https://doi.org/10.1089/apc.2017.0263
Graf, N., Dichtl, A., Deimel, D., Sander, D., & Stöver, H. (2018). Chemsex among men who have sex with men in Germany: Motives, consequences and the response of the support system. Sexual Health, 15(2), 151–156. https://doi.org/10.1071/SH17142
Grov, C., Rendina, H. J., Breslow, A. S., Ventuneac, A., Adelson, S., & Parsons, J. T. (2014). Characteristics of men who have sex with men (MSM) who attend sex parties: Results from a national online sample in the USA. Sexually Transmitted Infections, 90(1), 26–32. https://doi.org/10.1136/sextrans-2013-051094
Guerras, J. M., Hoyos Miller, J., Agustí, C., Chanos, S., Pichon, F., Kuske, M., Cigan, B., Fuertes, R., Stefanescu, R., Ooms, L., Casabona, J., de la Fuente, L., Belza, M. J., Fernández-Balbuena, S., Maté, T., Fernández, L., Platteau, T., Slaeen, P., Lixandru, M., & Cosic, M. (2020). Association of sexualized drug use patterns with HIV/STI transmission risk in an internet sample of men who have sex with men from seven European countries. Archives of Sexual Behavior, 50(2). https://doi.org/10.1007/s10508-020-01801-z
Hagan, H., Jordan, A. E., Neurer, J., & Cleland, C. M. (2015). Incidence of sexually transmitted hepatitis C virus infection in HIV-positive men who have sex with men. AIDS, 29(17), 2335–2345. https://doi.org/10.1097/QAD.0000000000000834
Hammoud, M. A., Bourne, A., Maher, L., Jin, F., Haire, B., Lea, T., Degenhardt, L., Grierson, J., & Prestage, G. (2018). Intensive sex partying with gamma-hydroxybutyrate: Factors associated with using gamma-hydroxybutyrate for chemsex among Australian gay and bisexual men-results from the Flux Study. Sexual Health, 15(2), 123–134. https://doi.org/10.1071/SH17146
Hampel, B., Kusejko, K., Kouyos, R. D., Böni, J., Flepp, M., Stöckle, M., Conen, A., Béguelin, C., Künzler-Heule, P., Nicca, D., Schmidt, A. J., Nguyen, H., Delaloye, J., Rougemont, M., Bernasconi, E., Rauch, A., Günthard, H. F., Braun, D. L., Fehr, J., …, & Yerly, S. (2020). Chemsex drugs on the rise: A longitudinal analysis of the Swiss HIV Cohort Study from 2007 to 2017. HIV Medicine, 21(4), 228–239. https://doi.org/10.1111/hiv.12821
Hegazi, A., Lee, M. J., Whittaker, W., Green, S., Simms, R., Cutts, R., Nagington, M., Nathan, B., & Pakianathan, M. R. (2017). Chemsex and the city: Sexualised substance use in gay bisexual and other men who have sex with men attending sexual health clinics. International Journal of STD and AIDS, 28(4), 362–366. https://doi.org/10.1177/0956462416651229
Heinsbroek, E., Glass, R., Edmundson, C., Hope, V., & Desai, M. (2018). Patterns of injecting and non-injecting drug use by sexual behaviour in people who inject drugs attending services in England, Wales and Northern Ireland, 2013–2016. International Journal of Drug Policy, 55, 215–221. https://doi.org/10.1016/j.drugpo.2018.02.017
Hibbert, M. P., Brett, C. E., Porcellato, L. A., & Hope, V. D. (2019). Psychosocial and sexual characteristics associated with sexualised drug use and chemsex among men who have sex with men (MSM) in the UK. Sexually Transmitted Infections, 95(5), 342–350. https://doi.org/10.1136/sextrans-2018-053933
Hockenhull, J., Murphy, K. G., & Paterson, S. (2017). An observed rise in γ-hydroxybutyrate-associated deaths in London: Evidence to suggest a possible link with concomitant rise in chemsex. Forensic Science International, 270, 93–97. https://doi.org/10.1016/j.forsciint.2016.11.039
Íncera-Fernández, D., Gámez-Guadix, M., & Moreno-Guillén, S. (2021). Mental health symptoms associated with sexualized drug use (chemsex) among men who have sex with men: A systematic review. International Journal of Environmental Research and Public Health, 18(24). https://doi.org/10.3390/IJERPH182413299
Ireland, G., Higgins, S., Goorney, B., Ward, C., Ahmad, S., Stewart, C., Simmons, R., Lattimore, S., & Lee, V. (2017). Evaluation of hepatitis C testing in men who have sex with men, and associated risk behaviours, in Manchester, UK. Sexually Transmitted Infections, 93(6), 404–409. https://doi.org/10.1136/sextrans-2016-052876
Kamal, R. M., van Noorden, M. S., Wannet, W., Beurmanjer, H., Dijkstra, B. A. G., & Schellekens, A. (2017). Pharmacological treatment in γ-hydroxybutyrate (GHB) and γ-butyrolactone (GBL) dependence: Detoxification and relapse prevention. CNS Drugs, 31(1), 51–64. https://doi.org/10.1007/s40263-016-0402-z
Karila, L., & Reynaud, M. (2011). GHB and synthetic cathinones: Clinical effects and potential consequences. In Drug Testing and Analysis (Vol. 3, Issue 9, pp. 552–559). Drug Test Anal. https://doi.org/10.1002/dta.210
Karila, L., Lafaye, G., Scocard, A., Cottencin, O., & Benyamina, A. (2018). MDPV and α-PVP use in humans: The twisted sisters. Neuropharmacology, 134(Pt A), 65–72. https://doi.org/10.1016/J.NEUROPHARM.2017.10.007
Kenyon, C., Wouters, K., Platteau, T., Buyze, J., & Florence, E. (2018). Increases in condomless chemsex associated with HIV acquisition in MSM but not heterosexuals attending a HIV testing center in Antwerp, Belgium. AIDS Research and Therapy, 15(1). https://doi.org/10.1186/s12981-018-0201-3
Knoops, L., Van Amsterdam, J., Albers, T., Brunt, T. M., & Van Den Brink, W. (2022). Slamsex in The Netherlands among men who have sex with men (MSM): Use patterns, motives, and adverse effects. Sexual Health, 19(6). https://doi.org/10.1071/SH22140
Kohli, M., Hickson, F., Free, C., Reid, D., & Weatherburn, P. (2019). Cross-sectional analysis of chemsex drug use and gonorrhoea diagnosis among men who have sex with men in the UK. Sexual Health, 16(5), 464–472. https://doi.org/10.1071/SH18159
Lafortune, D., Blais, M., Miller, G., Dion, L., Lalonde, F., & Dargis, L. (2021). Psychological and interpersonal factors associated with sexualized drug use among men who have sex with men: A mixed-methods systematic review. Archives of Sexual Behavior, 50(2), 427–460. https://doi.org/10.1007/s10508-020-01741-8
Latini, A., Dona, M. G., Alei, L., Colafigli, M., Frasca, M., Orsini, D., Giuliani, M., Morrone, A., Cristaudo, A., & Zaccarelli, M. (2019). Recreational drugs and STI diagnoses among patients attending an STI/HIV reference clinic in Rome, Italy. Sexually Transmitted Infections, 95(8), 588–593. https://doi.org/10.1136/sextrans-2019-054043
Lawn, W., Aldridge, A., Xia, R., & Winstock, A. R. (2019). Substance-linked sex in heterosexual, homosexual, and bisexual men and women: An online, cross-sectional “Global Drug Survey” report. Journal of Sexual Medicine, 16(5), 721–732. https://doi.org/10.1016/j.jsxm.2019.02.018
Lea, T., Hammoud, M., Bourne, A., Maher, L., Jin, F., Haire, B., Bath, N., Grierson, J., & Prestage, G. (2019). Attitudes and perceived social norms toward drug use among gay and bisexual men in Australia. Substance Use and Misuse, 54(6), 944–954. https://doi.org/10.1080/10826084.2018.1552302
Li, C. W., Ku, S. W. W., Huang, P., Chen, L. Y., Wei, H. T., Strong, C., & Bourne, A. (2021). Factors associated with methamphetamine dependency among men who have sex with men engaging in chemsex: Findings from the COMeT study in Taiwan. International Journal of Drug Policy, 93. https://doi.org/10.1016/j.drugpo.2021.103119
Liao, Y., Johnson, M., Qi, C., Wu, Q., Xie, A., Liu, J., Yang, M., Huang, M., Zhang, Y., Liu, T., Hao, W., & Tang, J. (2018). Cue-induced brain activation in chronic ketamine-dependent subjects, cigarette smokers, and healthy controls: A task functional magnetic resonance imaging study. Frontiers in Psychiatry, 9(MAR). https://doi.org/10.3389/fpsyt.2018.00088
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., Clarke, M., Devereaux, P. J., Kleijnen, J., & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. In PLoS Medicine (Vol. 6, Issue 7). PLoS Med. https://doi.org/10.1371/journal.pmed.1000100
Lingford-Hughes, A., Patel, Y., Bowden-Jones, O., Crawford, M. J., Dargan, P. I., Gordon, F., Parrott, S., Weaver, T., & Wood, D. M. (2016). Improving GHB withdrawal with baclofen: Study protocol for a feasibility study for a randomised controlled trial. Trials, 17(1). https://doi.org/10.1186/s13063-016-1593-9
Lyons, T., Chandra, G., Goldstein, J., & Ostrow, D. G. (2010). Breaking the bond between stimulant use and risky sex: A qualitative study. Substance Abuse, 31(4), 224–230. https://doi.org/10.1080/08897077.2010.514240
Macgregor, L., Kohli, M., Looker, K. J., Hickson, F., Weatherburn, P., Schmidt, A. J., & Turner, K. M. E. (2021). Chemsex and diagnoses of syphilis, gonorrhoea and chlamydia among men who have sex with men in the UK: A multivariable prediction model using causal inference methodology. Sexually Transmitted Infections, 97(4), 282–289. https://doi.org/10.1136/sextrans-2020-054629
Mattison, A. M., Ross, M. W., Wolfson, T., Franklin, D., Grant, I., Atkinson, J. H., McCutchan, J. A., Marcotte, T. D., Wallace, M. R., Ellis, R. J., Letendre, S., Schrier, R., Heaton, R. K., Cherner, M., Rippeth, J., Jernigan, T., Hesselink, J., Masliah, E., Masys, D. R., …, & Deutsch, R. (2001). Circuit party attendance, club drug use, and unsafe sex in gay men. Journal of Substance Abuse, 13(1–2), 119–126. https://doi.org/10.1016/S0899-3289(01)00060-8
Maxwell, S., Shahmanesh, M., & Gafos, M. (2019). Chemsex behaviours among men who have sex with men: A systematic review of the literature. International Journal of Drug Policy, 63, 74–89. https://doi.org/10.1016/j.drugpo.2018.11.014
Melendez-Torres, G. J., Bourne, A., Reid, D., Hickson, F., Bonell, C., & Weatherburn, P. (2018). Typology of drug use in United Kingdom men who have sex with men and associations with socio-sexual characteristics. International Journal of Drug Policy, 55, 159–164. https://doi.org/10.1016/j.drugpo.2018.01.007
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674. https://doi.org/10.1037/0033-2909.129.5.674
Miltz, A., Lampe, F., McCormack, S., Dunn, D., White, E., Rodger, A., Phillips, A., Sherr, L., Sullivan, A. K., Reeves, I., Clarke, A., & Gafos, M. (2019). Prevalence and correlates of depressive symptoms among gay, bisexual and other men who have sex with men in the PROUD randomised clinical trial of HIV pre-exposure prophylaxis. BMJ Open, 9(12). https://doi.org/10.1136/bmjopen-2019-031085
Miltz, A. R., Rodger, A. J., Sewell, J., Gilson, R., Allan, S., Scott, C., Sadiq, T., Farazmand, P., McDonnell, J., Speakman, A., Sherr, L., Phillips, A. N., Johnson, A. M., Collins, S., & Lampe, F. C. (2021). Recreational drug use and use of drugs associated with chemsex among HIV-negative and HIV-positive heterosexual men and women attending sexual health and HIV clinics in England. International Journal of Drug Policy, 91. https://doi.org/10.1016/j.drugpo.2020.103101
Mimiaga, M. J., Reisner, S. L., Vanderwarker, R., Gaucher, M. J., O’Connor, C. A., Medeiros, M. S., & Safren, S. A. (2008). Polysubstance use and HIV/STD risk behavior among Massachusetts men who have sex with men accessing Department of Public Health mobile van services: Implications for intervention development. AIDS Patient Care and STDs, 22(9), 745–751. https://doi.org/10.1089/apc.2007.0243
Morse, B. L., & Morris, M. E. (2013). Toxicokinetics/toxicodynamics of g-hydroxybutyrate-ethanol intoxication: Evaluation of potential treatment strategies. Journal of Pharmacology and Experimental Therapeutics, 346(3), 504–513. https://doi.org/10.1124/jpet.113.206250
Nanín, J. E., Parsons, J. T., Bimbi, D. S., Grov, C., & Brown, J. T. (2006). Community reactions to campaigns addressing crystal methamphetamine use among gay and bisexual men in New York City. Journal of Drug Education, 36(4), 297–315. https://doi.org/10.2190/9818-1W43-1876-2062
Nimbi, F. M., Rosati, F., Esposito, R. M., Stuart, D., Simonelli, C., & Tambelli, R. (2021). Sex in chemsex: Sexual response, motivations, and sober sex in a group of Italian men who have sex with men with sexualized drug use. Journal of Sexual Medicine, 18(12), 1955–1969. https://doi.org/10.1016/j.jsxm.2021.09.013
Pakianathan, M. R., Lee, M. J., Kelly, B., & Hegazi, A. (2016). How to assess gay, bisexual and other men who have sex with men for chemsex. Sexually Transmitted Infections, 92(8), 568–570. https://doi.org/10.1136/sextrans-2015-052405
Parry, S., Curtis, H., & Chadwick, D. (2019). Psychological wellbeing and use of alcohol and recreational drugs: Results of the British HIV Association (BHIVA) national audit 2017. HIV Medicine, 20(6), 424–427. https://doi.org/10.1111/hiv.12744
Platteau, T., Pebody, R., Dunbar, N., Lebacq, T., Collins, B., Platteau, T., Pebody, R., Dunbar, N., Lebacq, T., & Collins, B. (2019). The problematic chemsex journey : A resource for prevention and harm reduction. Drugs and Alcohol Today, 19, 49–54. https://doi.org/10.1108/DAT-11-2018-0066
Prestage, G., Hammoud, M., Jin, F., Degenhardt, L., Bourne, A., & Maher, L. (2018). Mental health, drug use and sexual risk behavior among gay and bisexual men. International Journal of Drug Policy, 55, 169–179. https://doi.org/10.1016/j.drugpo.2018.01.020
Pufall, E. L., Kall, M., Shahmanesh, M., Nardone, A., Gilson, R., Delpech, V., Ward, H., Hart, G., Anderson, J., Azad, Y., Elford, J., Sullivan, A., Mercer, C., McOwan, A., Peck, J., Cassell, J., Musonda, J., & Bruton, J. (2018). Sexualized drug use (‘chemsex’) and high-risk sexual behaviours in HIV-positive men who have sex with men. HIV Medicine, 19(4), 261–270. https://doi.org/10.1111/hiv.12574
Remien, R. H., Stirratt, M. J., Nguyen, N., Robbins, R. N., Pala, A. N., & Mellins, C. A. (2019). Mental health and HIV/AIDS: The need for an integrated response. AIDS (London, England), 33(9), 1411–1420. https://doi.org/10.1097/QAD.0000000000002227
Rosińska, M., Gios, L., Nöstlinger, C., VandenBerghe, W., Marcus, U., Schink, S., Sherriff, N., Jones, A. M., Folch, C., Dias, S., Velicko, I., & Mirandola, M. (2018). Prevalence of drug use during sex amongst MSM in Europe: Results from a multi-site bio-behavioural survey. International Journal of Drug Policy, 55, 231–241. https://doi.org/10.1016/j.drugpo.2018.01.002
Rosner, B., Neicun, J., Yang, J. C., & Roman-Urrestarazu, A. (2021). Substance use among sexual minorities in the US – linked to inequalities and unmet need for mental health treatment? Results from the National Survey on Drug Use and Health (NSDUH). Journal of Psychiatric Research, 135, 107–118. https://doi.org/10.1016/j.jpsychires.2020.12.023
Schecke, H., Lea, T., Bohn, A., Köhler, T., Sander, D., Scherbaum, N., & Deimel, D. (2019). Crystal methamphetamine use in sexual settings among german men who have sex with men. Frontiers in Psychiatry, 10. https://doi.org/10.3389/fpsyt.2019.00886
Schmidt, A. J., Bourne, A., Weatherburn, P., Reid, D., Marcus, U., Hickson, F., & Network, E. M. I. S. (2016). Illicit drug use among gay and bisexual men in 44 cities: Findings from the European MSM Internet Survey (EMIS). International Journal of Drug Policy, 38, 4–12. https://doi.org/10.1016/j.drugpo.2016.09.007
Scholz-Hehn, A. D., Milin, S., Schulte, B., Reimer, J., Buth, S., & Schäfer, I. (2022). Substance use and chemsex in MSM - a latent class analysis. Journal of Drug Issues, 52(1), 83–96. https://doi.org/10.1177/00220426211040564
Schreck, B., Guerlais, M., Laforgue, E., Bichon, C., Grall-Bronnec, M., & Victorri-Vigneau, C. (2020). Cathinone use disorder in the context of slam practice: New pharmacological and clinical challenges. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.00705
Schreck, B., Victorri-Vigneau, C., Guerlais, M., Laforgue, E., & Grall-Bronnec, M. (2021). Slam practice: A review of the literature. In European Addiction Research (Vol. 27, Issue 3, pp. 161–178). Eur Addict Res. https://doi.org/10.1159/000511897
Sewell, J., Miltz, A., Lampe, F. C., Cambiano, V., Speakman, A., Phillips, A. N., Stuart, D., Gilson, R., Asboe, D., Nwokolo, N., Clarke, A., Collins, S., Hart, G., Elford, J., & Rodger, A. J. (2017). Poly drug use, chemsex drug use, and associations with sexual risk behaviour in HIV-negative men who have sex with men attending sexual health clinics. International Journal of Drug Policy, 43, 33–43. https://doi.org/10.1016/j.drugpo.2017.01.001
Stevens, O., Moncrieff, M., & Gafos, M. (2020). Chemsex-related drug use and its association with health outcomes in men who have sex with men: A cross-sectional analysis of antidote clinic service data. Sexually Transmitted Infections, 96(2), 124–130. https://doi.org/10.1136/SEXTRANS-2019-054040
Tan, R. K. J., Phua, K., Tan, A., Gan, D. C. J., Ho, L. P. P., Ong, E. J., & See, M. Y. (2021). Exploring the role of trauma in underpinning sexualised drug use (‘chemsex’) among gay, bisexual and other men who have sex with men in Singapore. International Journal of Drug Policy, 97. https://doi.org/10.1016/j.drugpo.2021.103333
Tan, R. K. J., Wong, C. M., Chen, M. I. C., Chan, Y. Y., Bin Ibrahim, M. A., Lim, O. Z., Chio, M. T. W., Wong, C. S., Chan, R. K. W., Chua, L. J., & Choong, B. C. H. (2018). Chemsex among gay, bisexual, and other men who have sex with men in Singapore and the challenges ahead: A qualitative study. International Journal of Drug Policy, 61, 31–37. https://doi.org/10.1016/j.drugpo.2018.10.002
Tomkins, A., Ahmad, S., Cannon, L., Higgins, S. P., Kliner, M., Kolyva, A., Ward, C., & Vivancos, R. (2018). Prevalence of recreational drug use reported by men who have sex with men attending sexual health clinics in Manchester, UK. International Journal of STD and AIDS, 29(4), 350–356. https://doi.org/10.1177/0956462417725638
Torres, T. S., Bastos, L. S., Kamel, L., Bezerra, D. R. B., Fernandes, N. M., Moreira, R. I., Garner, A., Veloso, V. G., Grinsztejn, B., & De Boni, R. B. (2020). Do men who have sex with men who report alcohol and illicit drug use before/during sex (chemsex) present moderate/high risk for substance use disorders? Drug and Alcohol Dependence, 209. https://doi.org/10.1016/j.drugalcdep.2020.107908
Trouiller, P., Velter, A., Saboni, L., Sommen, C., Sauvage, C., Vaux, S., Barin, F., Chevaliez, S., Lot, F., & Jauffret-Roustide, M. (2020). Injecting drug use during sex (known as “slamming”) among men who have sex with men: Results from a time-location sampling survey conducted in five cities, France. International Journal of Drug Policy, 79. https://doi.org/10.1016/j.drugpo.2020.102703
Van Hout, M. C., Crowley, D., O’Dea, S., & Clarke, S. (2019). Chasing the rainbow: Pleasure, sex-based sociality and consumerism in navigating and exiting the Irish Chemsex scene. Culture, Health and Sexuality, 21(9), 1074–1086. https://doi.org/10.1080/13691058.2018.1529336
Vaux, S., Chevaliez, S., Saboni, L., Sauvage, C., Sommen, C., Barin, F., Alexandre, A., Jauffret-Roustide, M., Lot, F., Velter, A., Friboulet, D., Lydié, N., Peytavin, G., & Robineau, O. (2019). Prevalence of hepatitis C infection, screening and associated factors among men who have sex with men attending gay venues: A cross-sectional survey (PREVAGAY), France, 2015. BMC Infectious Diseases, 19(1), 315. https://doi.org/10.1186/s12879-019-3945-z
Vu, N. T. T., Holt, M., Phan, H. T. T., La, L. T., Tran, G. M., Doan, T. T., Nguyen, T. N. N., & de Wit, J. (2017). The relationship between methamphetamine use, sexual sensation seeking and condomless anal intercourse among men who have sex with men in Vietnam: Results of a community-based, cross-sectional study. AIDS and Behavior, 21(4), 1105–1116. https://doi.org/10.1007/s10461-016-1467-x
Wang, Z., Yang, X., Mo, P. K. H., Fang, Y., Ip, T. K. M., & Lau, J. T. F. (2020). Influence of social media on sexualized drug use and chemsex among Chinese men who have sex with men: Observational prospective cohort study. In Journal of Medical Internet Research (Vol. 22, Issue 7). J Med Internet Res. https://doi.org/10.2196/17894
Wang, H., Jonas, K. J., & Guadamuz, T. E. (2023). Chemsex and chemsex associated substance use among men who have sex with men in Asia: A systematic review and meta-analysis. Drug and Alcohol Dependence, 243. https://doi.org/10.1016/J.DRUGALCDEP.2022.109741
Weatherburn, P., Hickson, F., Reid, D., Torres-Rueda, S., & Bourne, A. (2017). Motivations and values associated with combining sex and illicit drugs (chemsex) among gay men in South London: Findings from a qualitative study. Sexually Transmitted Infections, 93(3), 203–206. https://doi.org/10.1136/sextrans-2016-052695
Wong, N. S., Kwan, T. H., Lee, K. C. K., Lau, J. Y. C., & Lee, S. S. (2020). Delineation of chemsex patterns of men who have sex with men in association with their sexual networks and linkage to HIV prevention. International Journal of Drug Policy, 75. https://doi.org/10.1016/j.drugpo.2019.10.015
Funding
Open access funding is provided thanks to the UBA-Library of the University of Amsterdam agreement with Springer Nature.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics Approval
Ethics Approval for this study was not necessary.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Brunt, T.M., Graf, N., Deimel, D. et al. Mental Health Among Men Who Have Sex with Men Under the Influence of Psychoactive Substances: a Systematic Review. Int J Ment Health Addiction (2024). https://doi.org/10.1007/s11469-023-01230-8
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-023-01230-8