
Abstract
In the modern interventional treatment of degenerated saphenous vein grafts, the use of both bare metal and drug eluting stents have been described so far. Drug eluting balloons have been increasingly used in cases of in-stent restenosis and to some extent de novo stenosis of native coronary vessels. Based on pure logic approach, the use of drug eluting balloons in in-stent restenosis of the saphenous vein graft may be of great interest. Still, few high-quality data on this subject exist and no general recommendations can be made. This paper illustrates a typical case of a symptomatic late in-stent restenosis of a saphenous vein graft occurred 15 months after a percutaneous coronary intervention with implantation of two drug eluting stents. Intravascular ultrasound revealed a mixture of stent underexpansion and severe neointima. This was treated safely with a prolonged high pressure balloon dilatation followed by dilatation with a drug eluting balloon. The primary result was very good. During the intervention the patient remained asymptomatic and was discharged the next day on dual anti-platelet therapy. During the 10-month follow-up the patient remained asymptomatic. This case demonstrates the usefulness and clinical safety of drug eluting balloons in treating in-stent restenosis in the saphenous vein grafts.
Similar content being viewed by others


Introduction
Despite the ongoing clinical and technical development, in-stent restenosis (ISR) illustrates the most common treatment failure after coronary interventions, occurring in up to 15% of all interventional cases [1, 2]. This has been demonstrated, in turn, to be associated with worse patients’ outcome and higher mortality rates [3, 4].
Percutaneous coronary interventions (PCI) of the saphenous vein grafts (SVG) are known to have a higher risk of restenosis and cardiovascular events (as compared to PCI in native arteries) [5]. The overall benefit of using saphenous vein grafts has been critically discussed as approximately half of the grafts remain occluded within the first 10 years after bypass surgery. This may be attributed to acute thrombosis, vascular inflammation, and accelerated atherosclerosis [6]. The data regarding the proper interventional treatment of SVG are very limited. In the DIVA trial, for instance, no relevant differences were found between the DES and BMS patients over a 12-month follow-up [7].
In case of any ISR, the current guidelines recommend new-generation DES and/or drug-eluting balloons [8]. Whereas most available data apply to native arteries, not large high-quality data concerning the optimal management of ISR in SVG exist.
This paper describes a typical case of symptomatic late ISR in the SVG due to a mixture of stent underexpansion and neointima presence.
Case Presentation
A male patient, aged 54, was referred to our institution to undergo a diagnostic coronary angiography. The gentleman complained of typical angina pectoris CCS 3 for 4 weeks. The referring cardiologist diagnosed a slightly reduced ejection fraction (LVEF 45%) with new inferior hypokinesia but without relevant structural abnormalities (LVEDD 52 mm, LVEDS 24 mm, LAD 38 mm, IVSd 11 mm).
The medical history encompassed, apart from well-controlled hypertension, diabetes on insulin and hyperlipidemia, a severe coronary three-vessel disease with prior coronary artery bypass grafting (2017, LIMA to LAD, RITA as T graft to CX, and single venous graft to the distal RCA). During the coronary angiography in 2021 due to suspected progressive disease (angina pectoris CCS 2 and anterior ischemia over 10% on the myocardial scintigraphy), chronic obstruction of arterial grafts and native RCA were revealed (with the patent saphenous graft). The native LAD and CX were treated with a balloon dilatation and three drug eluting stents were implanted according to the then guidelines. A possible re-surgery was discussed with the patient, but the patient did not give formal content and insisted on the interventional treatment. The last coronary angiography was performed in 2022 due to unstable angina pectoris and showed a very good result of the LAD and CX stents, but a subtotal obstruction of the proximal part of the saphenous graft to the RCA. This was treated successfully with direct implantation of two drug eluting stents in the suck-U-surge technique.
On the diagnostic coronary angiogram, a subtotal in-stent stenosis of the proximal part of the saphenous graft to the RCA with TIMI 1 flow was diagnosed (Fig. 1). Both the LAD and CX showed a very good long-term PCI result. The native RCA showed a very long (> 50 mm) proximal chronic in-stent occlusion, with a blunt proximal cap, severe calcification, and complex anatomy (J-CTO score with at least 4 points). At this stage, a decision was taken to re-treat the saphenous graft and, in case of PCI failure, to perform the recanalization of the native RCA.

Functional subtotal in-stent obstruction of the venous RCA graft
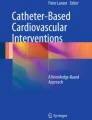
After successful wiring the distal vessel (Runthrough guidewire, Terumo), intravascular ultrasound was planned but failed due to subtotal occlusion. After a single balloon dilatation (Quantum Apex, Boston, NC 3,0 × 20 mm, 16 atm, 10 s) and implementation of a second wire (“buddy wire technique”; Runthrough guidewire), IVUS (Eagle Eye Platinum, Philips) was possible and revealed the underlying mechanism of the late in-stent stenosis: a mixture of stent underexpansion and neoatherosceloris (Fig. 2). This was treated with a prolonged high-pressure balloon dilation (Quantum Apex, Boston, NC 3.5 × 20 mm, 24 atm, 20 s; NC 4.0 × 20 mm, 24 atm, 20 s) followed by a dilatation with a drug-eluting balloon (SeQuent PleaseNeo, Braun, 4.0 × 20 mm, 12 atm, 60 s). The primary acute result was good, both on the angiogram and IVUS (Fig. 3). Post-PCI the patient stayed one night in the intermediate care unit and was discharged the next day on the dual antiplatelet therapy (for 6 months).

IVUS revealing a mixture of underexpansion and neoatherosceloris. MLA1 3.6 mm2 (diameter 2.0–2.3 mm) yellow line. MLA2 14.3 mm2 (diameter 4.1–4.5 mm) blue line. Plaque burden 74.8%

The primary result of DEB (angiography and IVUS). MLA1 7.8 mm2 (diameter 3.1–3.2 mm) yellow line. MLA 2 14.2 mm2 (diameter 4.2-.4.3 mm) blue line. Plaque burden 45%
The follow-up was taken over by the referring cardiologist. In the following 10 months, the patient has remained asymptomatic. The echocardiography revealed a normal ejection fraction (LVEF 55%) and no regional motion abnormalities were detected. The treadmill testing up to 150 W demonstrated no pathological reaction.
Discussion
In-stent restenosis in the SVG occurs in up to 21% of cases [9]. The late ISR seems to be dominated by various biological patterns including chronic inflammation accelerated neoatherosclerosis [10]. The proper management of this condition has not been established so far. Worse still, clinical event rates after any ISR intervention in the SVG are usually high and may be associated with poorer prognosis [2].
From the practical point of view, the interventional management of lesions in the SVG may be extremely challenging due to high rates of distal embolization and no reflow. The routine use of distal protection devices has been demonstrated to bring no benefit [6]. Certain unique techniques such as suck-U-surge method were described and can be useful in selected cases [11]. The pre- and/or post-conditioning with GP IIB/IIIa inhibitors such as eptifibatide was used in the past but its general efficacy and safety could not be demonstrated in larger groups [3]. The issue of ISR in the SVG may increase the complexity of the possible treatment strategies. One possible strategy is the use a scoring or cutting balloon: one study showed the lower rates of ISR compared with a conventional angioplasty prior to a drug eluting balloon [12]. Whereas scoring balloons usually do prevent balloon slippage, their deliverability is limited due to higher geometrical profile [12].
The current patient remains a typical DIVA trial individual: young, male, and without heart failure symptoms. Furthermore, the non-occlusive SVG lesion was developed within a drug-eluting stent and the TIMI 3 flow was present [7]. The DIVA trial showed a 19% occurrence of the primary outcome (i.e., targets vessel failure: death, myocardial infarction, or revascularization) in the patients treated with DES during a 12-month follow-up.
In case of stent underexpansion, a high-pressure balloon dilatation is usually performed to correct the failure and provide the optimal result. One of the most devastating complications of this approach is the perforation risk, followed by an obstructive shock due a possible pericardium effusion and tamponade [2]. This potential lethal complication must be treated with an emergent pericardiocentesis. In post-CABG patients, however, this may be challenging due to post-operative anatomical and structural changes.
The reported case illustrates that the use of drug eluting balloons seems to be a safe and effective treatment option. During the prolonged dilatation the patient remained asymptomatic. Neither hemodynamic deterioration nor slow flow was observed.
Code Availability
Not applicable.
Data Availability
On special request, all the collected data can be available.
Abbreviations
- BMS:
-
Bare metal stent
- CCS:
-
Canadian Cardiovascular Society
- CX:
-
Circumflex artery
- DES:
-
Drug eluting stent
- ISR:
-
In-stent restenosis
- IVUS:
-
Intravascular ultrasound
- J-CTO:
-
Japanese chronic total occlusion score
- LAD:
-
Left anterior descending artery
- LIMA:
-
Left internal mammary artery
- LVEDD:
-
Left ventricular end diastolic diameter
- LVESD:
-
Left ventricular end systolic diameter
- MLA:
-
Minimum lumen area
- NC:
-
Non-compliant
- RCA:
-
Right coronary artery
- RITA:
-
Right internal mammary artery
- SVG:
-
Saphenous vein graft
References
Jsselmuiden AJJ, Simsek C, van Driel AG, Bouchez D, Amoroso G, Vermeersch P, Karjalainen PP. Comparison between the STENTYS self- apposing bare metal and paclitaxel-eluting coronary stents for the treatment of saphenous vein grafts (ADEPT trial). Neth Heart J. 2018;26(2):94–101. https://doi.org/10.1007/s12471-017-1066-0.
Lichtenwalter C, de Lemos JA, Roesle M, Obel O, Holper EM, Haagen D, Saeed B, Iturbe JM, Shunk K, Bissett JK, Sachdeva R, Voudris VV, Karyofillis P, Kar B, Rossen J, Fasseas P, Berger P, Banerjee S, Brilakis ES. Clinical presentation and angiographic characteristics of saphenous vein graft failure after stenting: insights from the SOS (stenting of saphenous vein grafts) trial. JACC Cardiovasc Interv. 2009;2(9):855–60. https://doi.org/10.1016/j.jcin.2009.06.014.
Xenogiannis I, Rangan BV, Uyeda L, Banerjee S, Edson R, Bhatt DL, Goldman S, Holmes DR Jr, Rao SV, Shunk K, Mavromatis K, Ramanathan K, Bavry AA, McFalls EO, Garcia S, Thai H, Uretsky BF, Latif F, Armstrong E, Ortiz J, Jneid H, Liu J, Aggrawal K, Conner TA, Wagner T, Karacsonyi J, Ventura B, Alsleben A, Lu Y, Shih MC, Brilakis ES. In-stent restenosis in saphenous vein grafts (from the DIVA Trial). Am J Cardiol. 2022;1(162):24–30. https://doi.org/10.1016/j.amjcard.2021.09.024.
Xenogiannis I, Zenati M, Bhatt DL, Rao SV, Rodés-Cabau J, Goldman S, Shunk KA, Mavromatis K, Banerjee S, Alaswad K, Nikolakopoulos I, Vemmou E, Karacsonyi J, Alexopoulos D, Burke MN, Bapat VN, Brilakis ES. Saphenous vein graft failure: from pathophysiology to prevention and treatment strategies. Circulation. 2021;144(9):728–45. https://doi.org/10.1161/CIRCULATIONAHA.120.052163.
Mehran R, Dangas G, Abizaid AS, Mintz GS, Lansky AJ, Satler LF, Pichard AD, Kent KM, Stone GW, Leon MB. Angiographic patterns of in-stent restenosis: classification and implications for long-term outcome. Circulation. 1999;100(18):1872–8. https://doi.org/10.1161/01.cir.100.18.1872.
Colleran R, Kufner S, Mehilli J, Rosenbeiger C, Schüpke S, Hoppmann P, Joner M, Mankerious N, Fusaro M, Cassese S, Abdel-Wahab M, Neumann FJ, Richardt G, Ibrahim T, Schunkert H, Laugwitz KL, Kastrati A, Byrne RA, ISAR- CABG Investigators. Efficacy over time with drug-eluting stents in saphenous vein graft lesions. J Am Coll Cardiol. 2018;71(18):1973–82. https://doi.org/10.1016/j.jacc.2018.03.456.
Brilakis ES, Edson R, Bhatt DL, Goldman S, Holmes DR Jr, Rao SV, Shunk K, Rangan BV, Mavromatis K, Ramanathan K, Bavry AA, Garcia S, Latif F, Armstrong E, Jneid H, Conner TA, Wagner T, Karacsonyi J, Uyeda L, Ventura B, Alsleben A, Lu Y, Shih MC, Banerjee S, DIVA Trial Investigators. Drug- eluting stents versus bare-metal stents in saphenous vein grafts: a double- blind, randomised trial. Lancet. 2018;391(10134):1997–2007. https://doi.org/10.1016/S0140-6736(18)30801-8.
LinL,LuW,WangX,PanL,WangX,ZhengX,LiR,ShanY,PengM,QiuC. Short-term outcomes of drug-coated balloon versus drug-eluting stent for de novo saphenous vein graft lesions in coronary heart disease. Front Cardiovasc Med. 2023;10:982880. https://doi.org/10.3389/fcvm.2023.982880
Kuna C, Wiedenmayer N, Bradaric C, Presch A, Voll F, Kufner S, Ibrahim T, Schunkert H, Laugwitz KL, Cassese S, Kastrati A, Wiebe J. Ten-year outcomes after percutaneous coronary intervention of in-stent restenosis in saphenous vein grafts. Catheter Cardiovasc Interv. 2023;102(4):646–54. https://doi.org/10.1002/ccd.30807.
Wolny R, Mintz GS, Matsumura M, Ishida M, Fan Y, Fall KN, Parikh MA, Rabbani LE, Ali ZA, Karmpaliotis D, Kirtane AJ, Moses JW, Maehara A. Intravascular ultrasound assessment of in-stent restenosis in saphenous vein grafts. Am J Cardiol. 2019;123(7):1052–9. https://doi.org/10.1016/j.amjcard.2018.12.030.
Resch M, Ostheim P, Endemann DH, Debl K, Buchner S, Birner C, Maier LS, Kerber S, Luchner A, Griese DP. Drug coated balloon is less effective for treatment of DES in-stent restenosis both in native coronary arteries and saphenous vein grafts: results from a bicenter registry. J Interv Cardiol. 2016;29(5):461–8. https://doi.org/10.1111/joic.12324.
Kufner S, Joner M, Schneider S, Tolg R, Zrenner B, Repp J, Starkmann A, Xhepa E, Ibrahim T, Cassese S, Fusaro M, Ott I, Hengstenberg C, Schunkert H, Abdel-Wahab M, Laugwitz KL, Kastrati A, Byrne RA, Investigators I-D. Neointimal modification with scoring balloon and efficacy of drug-coated balloon therapy in patients with restenosis in drug-eluting coronary stents: a randomized controlled trial. JACC Cardiovasc Interv. 2017;10:1332–40.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
MR: main conception of the paper, wrote the paper, and performed the literature search. KK: contributed to the main theoretical background, verified the literature search, and supervised the project. All authors discussed the results and contributed to the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
No applicable.
Consent to Participate
Not applicable.
Consent for Publication
Written consent for publication was obtained from the patient and is available on request.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Medicine
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rogowski, M.M., Kara, K. Late In-Stent Restenosis of a Saphenous Vein Graft Treated with High-Pressure Balloon Dilatation and Drug Eluting Balloon Dilatation: Case Report. SN Compr. Clin. Med. 6, 10 (2024). https://doi.org/10.1007/s42399-023-01636-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s42399-023-01636-4