
Abstract
This study aimed to investigate the relationships between symptoms of study addiction and their relationships with dimensions of study engagement. We used two samples in which study addiction was measured with the Bergen Study Addiction Scale and study engagement was measured with the Utrecht Work Engagement Scale for Students. The samples comprised Norwegian (n = 1107) and Polish (n = 776) students. The networks featured three clusters of nodes (two clusters of the study addiction symptoms and one cluster of the study engagement dimensions). Study addiction clusters were connected with study engagement cluster through positive edges between absorption and study addiction symptoms, negative edges which vigor shared with conflict and problems, and negative edge between dedication and mood modification. Among the symptoms of study addiction, problems, conflict, and withdrawal were the most central and salience, tolerance, and mood modification were the least central. Moreover, conflict was the most predictable and relapse was the least predictable symptom of study addiction. The results from the present study are similar to those of previous studies on work addiction and support the notion that study addiction may be a precursor to work addiction. Although based on cross-sectional data, the nuanced differences between work addiction and study addiction networks are discussed as they lay a foundation for further investigation of the potential differences in transition mechanisms from healthy engagement to compulsive behavior.
Similar content being viewed by others


School and academic pressures have been growing the last decades (Cosma et al., 2022; Klinger et al., 2015). Such pressure is associated with declines in well-being among adolescents and young adults (De Looze et al., 2020; Pascoe et al., 2020) as well as widespread phenomena such as educational burnout (Kaggwa et al., 2021; Walburg, 2014). Increasing demands on students may push them into complete focus on studying to the exclusion of other developmental challenges relevant to their age group, particularly the development of close and mature social relationships, friendships, emotional self-regulation, and healthy self-image, in addition to individual passions and spare time activities (Atroszko & Atroszko, 2020a). “Study addiction” (Atroszko, 2013), “compulsive study behavior” (Woropay-Hordziejewicz et al., 2022), and “studyholism” (Loscalzo & Giannini, 2018a) are terms used to describe the phenomenon of problematic overstudying. Since student learning and associated coursework can be considered work (Griffiths et al., 2018), problematic overstudying has been conceptualized as an early form of work addiction (Atroszko, 2015, 2022a, 2022b). Study and work addiction share the following: (i) phenomenological manifestation (appetitive effects, distinctive craving, loss of control, and withdrawal symptoms; cf., Sussman, 2012), (ii) characteristic risk factors (e.g., perfectionism and family dynamics), (iii) specific comorbidities (e.g., eating disorders; Woropay-Hordziejewicz et al., 2022), (iv) distinctive consequences (e.g., health problems due to stress associated with extended mental work), and temporal stability (Atroszko et al., 2016a; for a detailed comparison see Atroszko, 2022a). Work addiction is associated with previous study addiction in longitudinal studies (Atroszko et al., 2016b).
The aim of this study was to investigate whether the structure of symptoms of study addiction is analogous to the structure of symptoms of work addiction. Furthermore, the goal was to inquire whether study engagement components are associated with study addiction similarly to relationships between work engagement and work addiction components. If data substantiated this, it would lend support to the hypothesis that study addiction represents an early form of work addiction, and that the two constructs share a similar mechanism of transition from healthy engagement to compulsive behavior.
Some researchers theorize that problematic overstudying might be a reflection of obsessive-compulsive disorder (Loscalzo & Giannini, 2018a). However, several factors are inconsistent with this hypothesis: (i) study addiction lacks characteristics typical for obsessive-compulsive disorders and behaviors (Atroszko, 2019), (ii) study addiction refers to planned behavior involving higher-order cognitive processes and attempts to achieve some appetitive effect and satiation through engagement in it (cf. Sussman, 2012; Sussman & Sussman, 2011), and (iii) study addiction manifests with typical addiction symptoms of craving, loss of control, withdrawal, tolerance, and obsession (Atroszko, 2022b). Moreover, (iv) about one-third of students manifesting all study addiction symptoms have low and very low levels of obsessive-compulsive personality disorder (OCPD) symptomatology (Atroszko et al., 2023b). Perfectionism associated with OCPD may still be a strong risk factor in many cases, analogously to work addiction (Atroszko et al., 2020); however, all these premises suggest that problematic overstudying can be viewed as an addictive disorder/problem and measured as such.
Previous studies show that study addiction is associated with a wide range of disadvantageous phenomena, including lower general health, lower quality of life, poor sleep, loneliness, less perceived support from friends, high perceived stress and exam stress, high cardiovascular reactivity to stress in situations of academic evaluation, high competitiveness component of Type A Personality which is associated with cardiovascular risk, neuroticism, psychasthenia, narcissism, pessimism, and worse academic performance (Atroszko, 2015; Atroszko et al., 2019; for an overview, see Atroszko, 2022a, 2022b). Study addiction is associated with other psychopathologies, including depression and anxiety, social anxiety, and eating disorders (Atroszko, 2015; Lawendowski et al., 2020; Woropay-Hordziejewicz et al., 2022), as well as other addictive behaviors related to food intake, social networking sites usage, shopping, gaming, and pornography (Atroszko et al., 2021; Charzyńska et al., 2021).
More nuanced analyses show that study addiction is associated with maladaptive perseverance (Czerwiński et al., 2023). Similarly, social anxiety is associated with impaired academic performance but only among those who have high study addiction (Lawendowski et al., 2020). These findings lend support to the notion that study addiction is clearly a negative and counterproductive phenomenon. Moreover, they support the model of study addiction as a result of ineffective stress-coping strategy (Atroszko, 2015) in which increased effort and perseverance among those who struggle with other problems in life (such as social anxiety) gradually turns into compulsion and leads to narrowing down of life interests and sources of pleasure. The increasing priority given to study behavior to the extent that it takes precedence over other life interests and daily activities is a core symptom of addiction (c.f., World Health Organization, 2019).
The current study will provide data on the structure of symptoms of study addiction and components of learning engagement, elucidating potential mechanisms of transition from healthy passion towards learning to compulsive behavior. While it is based on cross-sectional data, it will still allow for narrowing down and testing hypotheses concerning these mechanisms, which can be subsequently investigated with longitudinal designs.
Study addiction shows a similar prevalence to work addiction (Andersen et al., 2023). It seems to be among the most prevalent addictive behaviors and has higher prevalences when compared to gaming, shopping, food, pornography, and social networking sites addiction in the same sample of students and using a similar methodology for prevalence estimation (Atroszko et al., 2021; see Moskalewicz et al., 2019). The available estimates of study addiction suggest prevalences ranging from about 6 to 17% depending on country and sample type (Atroszko et al., 2019 for an overview, see Atroszko, 2022a). However, more recent analyses suggest that these rates may reflect overestimations because of the imperfect cut-off applied (Atroszko et al., 2023a; Bereznowski & Konarski, 2020). Studies with improved cut-off methodology conducted on nationally representative samples are necessary to evaluate the scale of this problem worldwide.
The Bergen Study Addiction Scale (BStAS; Atroszko et al., 2015) has proved to be a valid and reliable measure that assesses seven components of study addiction (i.e., salience, tolerance, mood modification, relapse, withdrawal, conflict, and problems; see Griffiths, 2005). It is based on the Bergen Work Addiction Scale (BWAS; Andreassen et al., 2012) which reflects the same components of addiction. It has been used among undergraduate and high school students worldwide, including in Poland, Norway, Turkey, Germany, Italy, Portugal, the USA, and India (Atroszko et al., 2015; Atroszko, Buźniak, et al., 2023a; Bisht & Godiyal, 2016; Charzyńska et al., 2021; Czerwiński et al., 2023; Godzwon et al., 2022; Kircaburun et al., 2021; Kozak et al., 2020; Lawendowski et al., 2020; Loscalzo & Giannini, 2018b; Schaefer & Strob, 2023; Wróbel, 2020).
BStAS scores correlate positively with learning engagement (Atroszko, 2015; Atroszko et al., 2015; Czerwiński et al., 2023; Lawendowski et al., 2020; Wróbel, 2020) and its components, especially with absorption (Atroszko & Atroszko, 2019). High time and effort involvement characteristic of both phenomena, to a large degree, account for these associations. Nonetheless, studies show that learning engagement is positively related to well-being and academic/school performance, whereas study addiction is linked to deteriorated psychosocial functioning (Atroszko, 2022b). Moreover, the absorption component of engagement may be a doorway to addiction because it phenomenologically is very similar to the experience of the “high” obtained with drugs. When students are absorbed in studying, they feel elated, and while fully focused, they forget about everything else and may have difficulties detaching from studying. Among individuals at risk, this gratifying experience may lead to the development of compulsive behavior because they may use this “high” produced by studying to escape from difficult emotions, stress, and other life problems (Jouhki & Oksanen, 2022). This mechanism is supported in network analysis studies of the structure of work addiction symptoms, work engagement components, stress, and burnout (Bereznowski et al., 2023a).
Previous studies in Norway and Poland used a network analytic approach to investigate the structure of components of work addiction measured with the BWAS. They showed two clusters of symptoms. Cluster 1 included tolerance, relapse, conflict, and problems, and Cluster 2 included salience, mood modification, and withdrawal (Bereznowski et al., 2022). Relapse had the highest network centrality. It was operationalized as the extent to which others told an individual to cut down on work without listening to them. It could represent its essential role as a diagnostic criterion. Work addiction is likely best identified when people close to those addicted recognize and communicate their overinvolvement in work.
On the other hand, mood modification had the lowest network centrality and predictability (Bereznowski et al., 2022), which likely represents its nature as a bridge linking healthy engagement with addiction (Bereznowski, Atroszko, & Konarski, 2023a). Conflict had the highest predictability in the networks, showing that other symptoms of addiction may affect it to the most significant degree. This finding is congruent with the notion that work addiction fuels work/life conflict (Clark et al., 2016), leading to a host of negative consequences for the addicted individuals and people around them (Atroszko & Atroszko, 2020b), including colleagues at work, subordinates, recipients of work, and in family, particularly children, and friends (Atroszko, 2022a)
Network analyses have been conducted to investigate associations of work addiction symptoms with work engagement dimensions of absorption, dedication, and vigor (Bereznowski, Atroszko, & Konarski, 2023a; Bereznowski, Bereznowska, et al., 2023b). The results suggest that the absorption dimension of work engagement and the mood modification component of work addiction could constitute a bridge between healthy engagement and addiction to work. Mood modification and absorption had the highest centrality in the networks based only on edges with other phenomena. Vigor was negatively related to mood modification, conflict, and problems showing that this dimension of engagement is clearly positive and opposite to central addiction symptoms. Dedication was positively related to tolerance and negatively linked to mood modification, suggesting that it is associated with a tendency to do more work but not regulated by a typical addictive mechanism of emotional escapism but rather by positive feelings of being devoted to work.
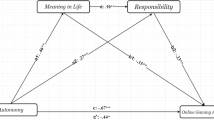
Based on the assumption that study addiction is an early form of work addiction and that mechanisms of transition between healthy engagement and addiction are analogous in the domains of studying and working, it can be expected that structures of networks of study addiction and study engagement will correspond to previously reported results found in research on work engagement and addiction networks (Bereznowski et al., 2022; Bereznowski, Bereznowska, et al., 2023b). Most importantly, the structures will reflect the hypothetical transition process from engagement to addiction via absorption and mood modification components (see Fig. 1). Against this backdrop, we conducted a network analysis study investigating the relationship between study addiction and work addiction symptoms in two samples of students. The following hypotheses were posited:

The visual representation of the hypothetical transition process from engagement to addiction via the absorption component of engagement and mood modification symptom of addiction
Hypotheses
Hypothesis 1: The study addiction networks will have a topology similar to the work addiction networks, which will be observable by the following:
-
H1A: The study addiction networks will include two clusters of symptoms (cluster 1: tolerance, relapse, conflict, and problems; cluster 2: salience, mood modification, and withdrawal).
-
H1B: Relapse will have the highest centrality and mood modification will have the lowest centrality in the study addiction networks.
-
H1C: Conflict will have the highest predictability and mood modification will have the lowest predictability in the study addiction networks.
Hypothesis 2: The study addiction and study engagement network will have topologies similar to the work addiction and work engagement network, which will be observable by the following:
-
H2A: The study addiction and study engagement networks will include three clusters of nodes (two clusters of study addiction symptoms (see H1A) and one cluster of study engagement dimensions).
-
H2B: Absorption will be positively related to all symptoms of study addiction.
-
H2C: Vigor will be negatively related to mood modification, conflict, and problems.
-
H2D: Dedication will be positively related to tolerance and negatively related to mood modification.
-
H2E: Mood modification and absorption will have the highest centrality (based only on edges with other phenomena) in the study addiction and study engagement networks.
Method
Study Design
Data collection was based on convenience sampling and took place from September to December 2014 in Norway (Sample 1) and from October 2014 to January 2015 in Poland (Sample 2). The two samples were recruited as part of longitudinal study on study addiction (Atroszko et al., 2016a). The participants completed online surveys. They were invited to take part in the survey either via university e-mailing system or via an announcement on a university website. Participation was anonymous but each participant was eligible to participate in a gift cards raffle. There were 60 gift cards (500 NOK) for participants from Norway and 100 gift cards (50 PLN) for participants from Poland.
Ethics
The study was reviewed and approved by both the Norwegian Data Protection Official for Research and the Research Ethics Committee at the Psychology Department of the University of Gdańsk in Poland. Neither of these committees regarded attaining written informed consent as necessary as voluntary completion of the survey was regarded as providing consent.
Participants
The samples included responses from 1107 studying Norwegians and 776 studying Poles. In Norway, 806 women and 301 men participated, and their mean age was 24.49 years (SD = 4.37). In Poland, 640 women and 136 men took part, with a mean age of 22.01 years (SD = 1.71). Detailed demographic and study-related information about participants are presented in Table 1.
Measures
Participants were asked about basic demographic information (sex, age, and marital status) and basic study-related information (mode of study (full time vs. part time) and number of hours devoted to studying weekly).
Study Addiction
The Bergen Study Addiction Scale (BStAS; Atroszko et al., 2015) is a modified version of the Bergen Work Addiction Scale (BWAS; Andreassen et al., 2012) in which “work,” “working,” and “worked” are replaced with “study,” “studying,” and “studied” (e.g., “How often during the last year have you thought of how you could free up more time to study?”). This measure consists of seven items, one for each symptom of addiction (Griffiths, 2005). The respondents evaluated the frequency of each symptom over the past twelve months. Responses are provided on a 5-point Likert scale ranging from 1 (never) to 5 (always). The measure does not have a skip structure and the responses were not preprocessed in any way. The Norwegian and Polish versions showed good content, convergent, criterion, and factor validity in previous studies (Atroszko, 2015; Atroszko et al., 2015, 2016a, 2016b). In this study, the Cronbach’s alpha reliability coefficient were .81 in the Norwegian sample and .82 in the Polish sample, respectively.
Study Engagement
The Utrecht Work Engagement Scale for Students (UWES9-S; Schaufeli & Bakker, 2004) is a modified version of the Utrecht Work Engagement Scale (UWES9; Schaufeli et al., 2006). The items are rephrased in order to fit the studying context (e.g., “At my work, I feel bursting with energy” was rephrased to “When I’m doing my work as a student, I feel bursting with energy”). The UWES9-S consists of nine items, three for each dimension of study engagement: vigor, dedication, and absorption. The respondents evaluate the frequency of each statement in general (without a specified time frame). Responses are provided on a 7-point Likert scale ranging from 1 (never) to 7 (everyday). The measure does not have a skip structure. Responses were preprocessed by summing the scores of items representing each dimension (i.e., the items of UWES9-S were responsible for three nodes in the networks (vigor, dedication, and absorption)). The Norwegian and Polish versions of the UWES9 showed good content, convergent, criterion, and factor validity in previous studies (Nerstad et al., 2010; Pollak et al., 2017). In the present study, the Cronbach’s alpha reliability coefficient were 0.88 for vigor, 0.89 for dedication, and 0.87 for absorption in the Norwegian sample and 0.79 for vigor, 0.85 for dedication, and 0.76 for absorption in the Polish sample, respectively.
Statistical Analyses
We estimated two pairs of networks (i.e., four networks). In each of the pairs one of the samples were Norwegian and one Polish. In the first pair, we estimated the networks including study addiction symptoms only, and in the second pair, we estimated the networks including study addiction symptoms and study engagement dimensions. The analyses were performed in R version 4.2.2 (R Core Team, 2022), and the network’s visualizations were created with the qgraph 1.9.3 package (Epskamp et al., 2012). To report the results, we followed the guidelines set by Burger et al. (2022). The analytical code is available at https://osf.io/f5vsq/?view_only=ab6f0e77ce054c759fca0506a2ffe5bf.
Network Estimation
Each pair of networks was estimated jointly using fused graphic lasso (FGL) method and the EstimateGroupNetwork 0.3.1 package, which is the recommended method for joint network estimation (Costantini & Epskamp, 2017). The optimal values of the tuning parameters were selected via k-fold cross-validation with seed set to 1. Layouts for visualizations were based on the layouts calculated for networks of work addiction and work engagement in previous studies (Bereznowski et al., 2022; Bereznowski, Bereznowska, et al., 2023b). The clusters of nodes were identified with a spin-glass algorithm implemented in the igraph 1.4.1 package (Csardi & Nepusz, 2006). This exploratory algorithm was designed to detect the optimal number of clusters in the network (we did not change the default values of the parameters, which allow detection of up to 25 clusters).
Network Stability
The stability of the networks was evaluated with the bootnet 1.5 package (Epskamp et al., 2018), and its implementation of nonparametric bootstrapping and case bootstrapping was based on 1000 bootstrap samples. The stability of each network was measured with the correlation stability coefficient, which represents “the maximum proportion of cases that can be dropped, such that with 95% probability the correlation between original centrality indices and centrality of networks based on subsets is 0.7 or higher” (Epskamp et al., 2018, p. 200). The stability of the network is regarded as acceptable when the correlation stability coefficient exceeds 0.25 and as good when it exceeds 0.50 (Epskamp et al., 2018).
Network Inference
For all networks, we calculated the standard version of the node strength which is equal to the sum of absolute values of all edges connecting a given node with other nodes in the network. Additionally, for study addiction and study engagement networks, we calculated a modified version of the node strength which allows to better capture which nodes are responsible for bridges between different phenomena. The modified version of the node strength is equal to “the sum of absolute values of all edges of a given node to all other nodes which represent different psychological phenomenon” (Bereznowski, Bereznowska, et al., 2023b, p. 11; e.g., for vigor, edges between vigor and study addiction symptoms). In order to compare the pairs of networks with respect to both standard and modified version of the node strength, we calculated Spearman correlation coefficients.
For all networks, we estimated the predictability of nodes using the mgm 1.2–13 package (Haslbeck, 2019). For ordinal data (symptoms of study addiction), node predictability indicates how much a node “can be predicted by all other nodes in the network, beyond what is trivially predicted by the marginal distribution” (Haslbeck & Waldorp, 2018, p. 856). For continuous data (dimensions of study engagement), node predictability indicates the proportion of variance explained by all other nodes in the network.
Network Comparison
We used NetworkComparisonTest 2.2.1 package (van Borkulo et al., 2017) with a seed set to 1 to compare pairs of networks. We started with the omnibus test, which determines whether there are any differences between networks in terms of edge weights. When the omnibus test was significant, we performed the post hoc test (with Holm-Bonferroni correction) to identify which specific edges were different. Finally, we compared the pairs of networks with respect to global strength (the sum of all absolute edge weights in the network).
Results
Descriptive Statistics
Skewnesses, kurtoses, means, and standard deviations of the seven symptoms of study addiction and the three dimensions of study engagement are presented in Table 2. The skewnesses and kurtoses indicated that the study variables’ distributions deviated from the normal distribution. However, since a recent simulation study showed that transformation of skewed ordinal data has negligible effects on the performance of network estimators (Isvoranu & Epskamp, 2023), we decided not to apply any transformation. By this approach we enable our results to be directly comparable with the work addiction and work engagement studies in which the raw data were analyzed (Bereznowski et al., 2022; Bereznowski, Bereznowska, et al., 2023b).
Network Analysis
Study Addiction Networks
The two addiction networks were accurately estimated. Their correlation stability coefficients were 0.75 for Norway and 0.59 for Poland, both indicating good stability. The networks are visualized in Fig. 2. The network density equaled 0.90 (19/21 edges) in Norway and 0.86 (18/21 edges) in Poland. In both cases, the mean absolute edge weight equaled 0.11. The spin-glass algorithm identified two identical clusters in both networks. The first cluster included salience (1), mood modification (3), and withdrawal (5), and the second cluster included tolerance (2), relapse (4), conflict (6), and problems (7). These two clusters are identical to the clusters observed for work addiction (Bereznowski et al., 2022).

The regularized partial correlation networks of study addiction. The less (more) pathological symptoms of study addiction are represented by lighter (darker) gray nodes. Blue (red) lines represent positive (negative) edges. The strength of a relationship is represented by line thickness and darkness. The orange area in the ring around a node represents predictability based on a node’s marginal distribution. The red area represents predictability based on the variance of a symptom explained by its neighbors. 1 = salience; 2 = tolerance; 3 = mood modification; 4 = relapse; 5 = withdrawal; 6 = conflict; 7 = problems
In both networks, salience (1), tolerance (2), and mood modification (3) were among the least central symptoms, and withdrawal (5), conflict (6), and problems (7) were among the most central symptoms (standard version of the node strength; see Fig. 3). However, there were small variations between samples with respect to the exact order of point estimates of centrality for these symptoms. Spearman correlation coefficient of the standard version of the node strength equaled 0.82.

The unstandardized values of the standard version of the node strength in the study addiction networks
The average predictability equaled 19.3% in Norway and 21.6% in Poland (41.9% and 39.1%, respectively, when including marginal distributions). The most predictable symptom in Norway and Poland was conflict (6) with predictability equal to 18.2% and 21.7%, respectively. The least predictable symptom was mood modification (3) in Norway (7.8%) and relapse (4) in Poland (7.9%, while predictability of mood modification equaled 12.8%).
The omnibus test was statistically significant, p = 0.022. Five out of 21 edges (23.8%) differed significantly: salience (1)—tolerance (2), tolerance (2)—relapse (4), salience (1)—withdrawal (5), salience (1)—conflict (6), and withdrawal (5)—problems (7). The networks did not differ with respect to global strength, p = 0.314.
Study Addiction and Study Engagement Networks
The two addiction and engagement networks were accurately estimated. Their correlation stability coefficients were 0.67 for Norway, and 0.75 for Poland, both indicating good stability. The networks are visualized in Fig. 4. The network density equaled 0.47 (21/45 edges) in Norway and 0.56 (25/45 edges) in Poland. In both cases, the mean absolute edge weight equaled 0.10. The spin-glass algorithm identified two identical clusters in both networks. First cluster included the study addiction symptoms, and the second cluster included the study engagement dimensions.

The regularized partial correlation networks of study addiction and study engagement. The symptoms of study addiction are represented by gray nodes and the dimensions of study engagement are represented by blue nodes. Blue (red) lines represent positive (negative) edges. The strength of a relationship is represented by line thickness and darkness. In the case of symptoms of study addiction, the orange area in the ring around a node represents predictability based on the marginal distribution of a node and the red area represents predictability based on the variance of a symptom explained by its neighbors. In the case of dimensions of study engagement, the blue area in the ring around a node represents a proportion of variance explained (R2). 1 = salience; 2 = tolerance; 3 = mood modification; 4 = relapse; 5 = withdrawal; 6 = conflict; 7 = problems
In both networks salience (1) was the least central symptom of work addiction, whereas problems (7) was the most central symptom of work addiction, dedication (D) was the least central dimension of study engagement, whereas absorption (A) was the most central dimension (see Fig. 5A for standard version of the node strength and Fig. 5B for the modified version of the node strength). Spearman correlation coefficient equaled 0.95 for the standard version of the node strength and 0.94 for the modified version of the node strength.

A The unstandardized values of the standard version of the node strength in the study addiction and study engagement networks. B The unstandardized values of the modified version of the node strength in the study addiction and study engagement networks
The average predictability equaled 33.4% in Norway and 33.2% in Poland (57.0% and 54.7%, respectively, when including marginal distributions for symptoms). The most predictable symptom in Norway and Poland was conflict (6) with predictability equal to 20.7% and 23.0%, respectively. The least predictable symptom in Norway and Poland was relapse with predictability equal to 8.5% and 7.9%, respectively. Mood modification had predictability equal to 8.4% in Norway and 11.5% in Poland. The most predictable dimension in Norway and Poland was absorption (A), 67.0% (Norway) and 73.1% (Poland), whereas the least predictable dimension was vigor, 60.1% (Norway) and 50.7% (Poland).
The omnibus test was statistically significant, p < 0.001. Twelve out of 45 edges (26.7%) differed significantly: salience (1)—tolerance (2), tolerance (2)—relapse (4), salience (1)—withdrawal (5), withdrawal (5)—conflict (6), and withdrawal (5)—problems (7), conflict (6)—vigor (V), salience (1)—absorption (A), mood modification (3)—absorption (A), relapse (4)—absorption (A), conflict (6)—absorption (A), vigor (V)—absorption (A), and vigor (V)—dedication (D). The networks did not differ with respect to global strength, p = 0.619.
Discussion
The present study aimed to investigate the relationships between study addiction symptoms and study engagement components in the two samples with diverse cultural backgrounds. The networks in Poland and Norway were almost identical, with a few minor differences. For example, there was a weak association between salience and tolerance, and mood modification and absorption in Poland, while in Norway, there was none. While this may reflect cultural differences, it has to be emphasized that within the full complex nature of interrelationships between ten nodes and possible 90 edges and the overwhelming similarity of structures, the aforementioned differences are trivial and need further replication. These overall between-country resemblances parallel remarkable similarities found previously in work addiction networks in samples from different countries and of diverse sociodemographic makeup (Bereznowski et al., 2022; Bereznowski, Bereznowska, et al., 2023b).
Similar to the structure of work engagement and work addiction components, we identified three distinct clusters of nodes: one cluster for the dimensions of study engagement and two clusters for study addiction symptoms (H1A and H2A supported). Contrary to the expectations, relapse did not have the highest centrality (H1B not supported), but problems (7), conflict (6), and withdrawal (5) had relatively similar and highest centrality in both samples. These are very interesting results suggesting that compared to working populations, for students, being told by others to cut down on studying without listening to them is not as diagnostically central. It may be that it happens less often than in relation to work because studying is socially highly valued and praised, and spending long hours on it is expected by parents, teachers, and even peers. It is also conceivable that fewer students than workers are in a steady relationship, which, compared to workers would reduce the chances of interpersonal reactions to specific behaviors. In line with this, working too much may more directly conflict with other roles and obligations in life, such as family-related (Atroszko, 2022a; Clark et al., 2016; Robinson, 2014). Therefore, the problem of overworking may be more easily observed and recognized by others than the problem of overstudying. Instead, symptoms associated with negative consequences of study addiction (problems and conflict) and withdrawal had the highest centrality in Poland and Norway. It indicates that these may constitute core diagnostic criteria representing crucial addictive mechanisms and processes.
Mood modification (3), together with salience (1) and tolerance (2), had the lowest centrality in the study addiction networks (H2B partially substantiated). These symptoms may, to a larger degree, represent peripheral processes associated with a higher focus on studying in general, which may, to some extent, be associated with high study engagement or situational factors such as demands from the course, pressures from the environment or socioeconomic pressures (Atroszko, 2013). For a discussion on the differences between study addiction and non-compulsive forms of high study involvement, see Atroszko (2022b). Also, previous work has shown that items representing these symptoms, particularly item 1 (salience) and item 2 (tolerance), are less “diagnostic” in the study and work addiction scales across countries (Atroszko, Buźniak, et al., 2023a; Bereznowski & Konarski, 2020).
Conflict (6) had the highest predictability and mood modification (3) had one of the lowest predictabilities in the four networks (H1C mostly substantiated). The least predictable symptom in three out of the four networks was relapse (4), which was also among the least predictable symptoms of work addiction (Bereznowski et al., 2022). Together these results highlight subtle differences between study addiction and work addiction. These results also indicate that while conflict may arise as a consequence of other study addiction symptoms, the activation of symptoms such as mood modification and relapse is related to factors that are external to the process of addiction. Currently, the only known external factor co-occurring with mood modification is perceived stress, and no external factors co-occurring with relapse are known (Bereznowski, Atroszko, & Konarski, 2023a). Consequently, further work is needed to identify external key factors related to specific symptoms of both study addiction and work addiction.
Interestingly the strength of association between study addiction withdrawal and relapse is more similar to networks found in general populations of working people in Norway and Poland in comparison to those found among younger populations of recent graduates (Bereznowski et al., 2022). This may reflect the progressive nature of addiction and suggest that among undergraduate students, networks resemble more “mature” structures found in relatively older working populations. Hence, study addiction at this stage may result from a longer process that could have started already in high school or earlier (Wróbel, 2020). Future longitudinal studies may shed light on this hypothesis.
The study engagement cluster was connected to the study addiction clusters through the negative edges between vigor (V) and conflict (6) and problems (7) (H2C mostly supported) and positive edges between absorption (A) and all the addiction symptoms in Poland and all but with mood modification in Norway (H2B mostly supported). Unlike networks of work addiction and work engagement, mood modification was only associated positively with absorption (A) in Poland and negatively with dedication (D) in both samples (hypotheses H2D and H2E partially supported). These results indicate that lower energy (vigor) associated with studying co-occurs with internal and external conflicts caused by studying, and associated problems. Also, higher work absorption co-occurs with experiencing all or most addiction symptoms, and higher work dedication co-occurs with a lower tendency to regulate mood with studying. The engagement cluster was more connected to the salience, mood modification, and withdrawal cluster than the other addiction symptoms. This disproportion was similar but less pronounced than in the work addiction and work engagement networks (Bereznowski, Bereznowska, et al., 2023b). This supports the assumption that the first cluster represents less pathological symptoms of work addiction (Bereznowski et al., 2022; see also Charlton & Danforth, 2007).
The notable difference between the current networks and previously identified networks of work addiction and work engagement is the fewer associations between mood modification and engagement components, including the lack of association with absorption (A) in Norway. This may point to some important differences in how mood is regulated by studying compared to how it is modified by work. On the other hand, in both samples, absorption (A) had relatively strongest links to conflict (6). While absorption (A) still seems to be a bridge between engagement and addiction, in the case of studying, the mechanism may involve its more direct association with negative consequences and the less pronounced mediating role of mood regulation. Students engrossed in studying and fully focused on this activity may ignore other spheres of life in a way that leads to harmful outcomes regardless of whether studying relieves them from low mood (or whether they perceive that it does). It is highly congruent with systematic structural equation modeling studies showing that the tendency to escape from personal problems into studying is not directly associated with neglecting health problems, ignoring social relationships, and depression symptoms, but seems to be mediated by the compulsion component of addiction (Atroszko, 2015, 2022b). These studies also showed that pleasure derived from studying, akin to absorption, had much stronger direct effects on study compulsion than indirect effects via the tendency to escape personal problems by studying.
This mechanism seems to suggest that in relation to study addiction, pleasure and absorption related to studying are stronger risk factors than negative reinforcements in the form of avoiding difficult emotional states, at least at the self-report level. It may be that positive reinforcements and mood regulation related to positive emotions play more important roles than in work addiction, in which escapism motives are either more pronounced or mature adults are more aware of them. It is also likely that these findings are associated with the fact that young adults (and adolescents) have (i) limited insight into their emotion regulation strategies associated with studying, (ii) generally lower insight into their emotional states, and (iii) greater reward-related neural activation (Vijayakumar et al., 2018). All these processes are associated with the maturation of prefrontal regions implicated in cognitive control, emotion regulation, and motivational and affective processing, which are responsible for numerous adverse outcomes during adolescence (e.g., health-risking behaviors, substance abuse, and depression; Vijayakumar et al., 2018). In other words, for some students, studying may be a highly reinforcing activity, and they may not understand and have control in terms of how studying regulates their emotional states. This, however, requires further systematic studies, and the current and novel findings contribute to the foundation for future work in this area.
Practical Implications
Foremostly, the findings provide important knowledge that can guide the prevention of study addiction and likely future work addiction. Passion for learning is a factor that is desirable for the development of young people and should be fostered within educational settings. However, excessive absorption in studying among individuals with risk factors, such as emotional instability, tendency to experience anxiety, high rigid perfectionism, or social anxiety, may lead to compulsive studying and relevant sequelae. The results of the present study draw attention to the need for a more careful evaluation of whether high engrossment in studying among adolescents and young adults reflects a healthy passion for learning or serves other functions that may lead to addictive behavioral patterns.
Moreover, the observed differences between networks of study addiction/engagement and previous networks of work addiction/engagement (Bereznowski, Atroszko, & Konarski, 2023a; Bereznowski, Bereznowska, et al., 2023b), together with findings from research using SEM models (Atroszko, 2015), suggest that young people may have less insight into how studying regulates their mood. Specifically, they may more readily observe how it brings them enjoyment or satisfaction rather than how it may represent an escape from negative emotional states. This is particularly worrisome because it may considerably contribute to a gradual narrowing of interests and sources of pleasure, which is a core symptom of all addictions (World Health Organization, 2019). Especially at the initial stages of the addictive process, vulnerable individuals may choose studying for its positive reinforcement effects while neglecting social relationships, hobbies, and other activities (see Atroszko, 2022b). Perhaps only after facing the harmful severe consequences of their overstudying (e.g., physical or mental health problems, lost relationships, and loneliness) may some realize that studying have become too central to their life and that they are in a serious predicament with the inability to enjoy anything else.
Based on the current findings, two recommendations seem to be in order. Firstly, screening studies that include the absorption component of engagement may aid early identification of students at risk of study addiction and thus enable supporting them (e.g., guidance/supervision). Secondly, broad psychoeducational programs for the general population of students may emphasize a need for balanced multidimensional development that includes social, emotional, and physical competencies. Also, specific programs within educational settings that focus on developing a wide range of skills, including self-regulatory skills, may reduce not only the risk of study addiction but also other addictive disorders and mental health problems, and is in line with a transdiagnostic approach to prevention (Berking & Lukas, 2015). Especially, it is important to emphasize to young people that overreliance on a single source of pleasure or satisfaction in life may be a pathway to addiction and mental health problems. This may also be one of the focal points in therapy, i.e., working on the problematic beliefs centered around the notion that academic success or work success will automatically translate into lasting happiness and fulfilment.
Strengths and Limitations
The present study included two large samples from different countries of considerably different socioeconomic backgrounds. Study addiction and study engagement were measured with the same instrument (i.e., the BStAS and the UWES-S) in each sample, and the instruments were entirely analogous to measures of work addiction (BWAS) and work engagement (UWES) used in previous studies allowing for direct comparisons between study and work addiction/engagement networks. The dimensions of study engagement were measured with three items each, which should reduce bias related to the unreliability of single-item indicators. The estimated networks included the external field of study addiction symptoms (the external field includes conditions other than addiction symptoms; in this case, the components of study engagement; Borsboom, 2017). It addresses the problem of rare investigation of external fields of mental disorders in psychological networks (Fried, 2020). Consequently, the present study contributes to the literature on compulsive overstudying and behavioral addictions and, at the same time, enriches the still scant literature on the replicability of psychological networks (Borsboom et al., 2017; Forbes et al., 2017a, b) as well as the literature on the external fields of mental disorders.
In terms of limitations, the samples were predominantly female, non-representative, and only from two countries restricting the generalizability of the results to clinical populations and populations from other countries and cultures. The data were cross-sectional, which puts limitations on causal inferences. The different study addiction symptoms were measured with single items, which may bias estimates of network parameters. The analyses did not include other mental disorders and psychological constructs (e.g., educational stress and burnout). This may influence the direct relationships between study addiction symptoms and study engagement components.
Conclusions and Future Study Directions
The present study showed that the structure of networks of study addiction and study engagement are largely analogous to the previously identified structures of networks of work addiction and work engagement. It supports the notion that study addiction comprises an early form of work addiction. Absorption (part of engagement) showed multiple direct relationships with study addiction symptoms, and mood modification showed few direct relationships with study engagement dimensions. However, some important and interesting differences observed may lay a foundation for further investigation of the potential differences in transitional mechanisms (while taking into account that the current study is cross-sectional) from healthy engagement to compulsive behavior. First, mood modification showed fewer connections with engagement components, suggesting that, in the context of previous studies, positive reinforcements (rather than negative) and/or low insight into emotional self-regulation associated with developmental age (maturation of prefrontal cortex) play a more pronounced role in study addiction than in work addiction. Second, the lower centrality of relapse measured as the extent to which others told an individual to cut down on studying without listening to them suggests that there might be less recognition of the problem of overstudying by people close to them (parents, siblings, teachers, and friends) compared to overworking which more directly conflicts with other roles, such as family-related. Third, symptoms associated with negative consequences of study addiction (problems and conflict) and withdrawal may constitute core diagnostic criteria representing crucial addictive mechanisms and processes. Fourth, among undergraduate students, the strength of association between withdrawal and relapse resembles more “mature” structures found in networks of relatively older working populations. Hence, study addiction at this stage may result from a longer process that could have started already in high school or earlier.
All these findings are novel and open the door to further systematic investigations. Moreover, future studies should investigate networks including additional variables in the external field of study addiction symptoms such as educational burnout, educational stress, perfectionism, and other potential comorbid psychopathologies. Cross-validation of the investigated networks with different item wordings is necessary in order to increase the generalizability of the results and document the validity of networks. Also, studies in clinical samples as well as exploring sex differences in networks are highly warranted. These should include longitudinal designs to investigate whether cross-sectional data is a good representation of a dynamic process of addiction within individuals and to examine the direction of the relationships between engagement and addiction components using structural equation modeling frameworks.
References
Andersen, F. B., Djugum, M. E. T., Sjåstad, V., & Pallesen, S. (2023). The prevalence of workaholism: A systematic review and meta-analysis. Frontiers in Psychology, 14, 1252373. https://doi.org/10.3389/fpsyg.2023.1252373
Andreassen, C. S., Griffiths, M. D., Hetland, J., & Pallesen, S. (2012). Development of a work addiction scale. Scandinavian Journal of Psychology, 53(3), 265–272. https://doi.org/10.1111/j.1467-9450.2012.00947.x
Atroszko, P. A. (2013). Relationship between financial resources and home environment and students’ learning-related attitudes, beliefs and behaviors. Ad Alta: Journal of Interdisciplinary Research, 3, 7–10. http://www.magnanimitas.cz/ADALTA/0302/papers/A_atroszko.pdf.
Atroszko, P. A. (2015). The structure of study addiction: Selected risk factors and the relationship with stress, stress coping and psychosocial functioning (Unpublished doctoral dissertation). University of Gdańsk.
Atroszko, P. A. (2019). Response to: Loscalzo and Giannini (2018). A boon of incoherence: Insights on the relationship between study/work addiction and obsessive-compulsive personality disorder. Journal of Psychiatry and Clinical Psychology, 19(2), 237–243. https://doi.org/10.15557/PiPK.2019.0025
Atroszko, P. A. (2022a). Non-drug addiction: Addiction to work. In V. B. Patel & V. R. Preedy (Eds.), Handbook of substance misuse and addictions (pp. 2981–3012). Springer. https://doi.org/10.1007/978-3-030-67928-6_3-1
Atroszko, P. A. (2022b). Inventory for early screening of work addiction-related behaviors in high school and undergraduate students: Features and applications. In V. B. Patel & V. R. Preedy (Eds.), Handbook of substance misuse and addictions (pp. 3157–3198). Springer. https://doi.org/10.1007/978-3-030-67928-6_3-1
Atroszko, P. A., Andreassen, C. S., Griffiths, M. D., & Pallesen, S. (2015). Study addiction—A new area of psychological study: Conceptualization, assessment, and preliminary empirical findings. Journal of Behavioral Addictions, 4(2), 75–84. https://doi.org/10.1556/2006.4.2015.007
Atroszko, P. A., Andreassen, C. S., Griffiths, M. D., & Pallesen, S. (2016a). Study addiction: A cross-cultural longitudinal study examining temporal stability and predictors of its changes. Journal of Behavioral Addictions, 5(2), 357–362. https://doi.org/10.1556/2006.5.2016.024
Atroszko, P. A., Andreassen, C. S., Griffiths, M. D., & Pallesen, S. (2016b). The relationship between study addiction and work addiction: A cross-cultural longitudinal study. Journal of Behavioral Addictions, 5(4), 708–714. https://doi.org/10.1556/2006.5.2016.076
Atroszko, B., & Atroszko, P. A. (2020a). Educational pressure and development of study addiction, work addiction and other mental disorders. Ars Educandi, 17(17), 11–39. https://doi.org/10.26881/ae.2020.17.01
Atroszko, P. A., & Atroszko, B. (2020b). The costs of work-addicted managers in organizations: Towards integrating clinical and organizational frameworks. Amfiteatru Economic, 22(14), 1265–1282. https://doi.org/10.24818/EA/2020/S14/1265
Atroszko, P. A., & Atroszko, B. (2019). Type-A personality competitiveness component linked to increased cardiovascular risk is positively related to study addiction but not to study engagement. Current Science, 117(7), 1184. https://doi.org/10.18520/cs/v117/i7/1184-1188
Atroszko, P. A., Atroszko, B., & Charzyńska, E. (2021). Subpopulations of addictive behaviors in different sample types and their relationships with gender, personality, and well-being: Latent profile vs. latent class analysis. International Journal of Environmental Research and Public Health, 18, 8590. https://doi.org/10.3390/ijerph18168590
Atroszko, P. A., Buźniak, A., Woropay Hodziejewicz, N., Kierzkowski, M., & Lawendowski, R. (2023a). Identifying individual vulnerabilities and problematic behaviours hindering musicians’ development: Obsessive-compulsive personality disorder vs. study addiction. Musicae Scientiae. https://doi.org/10.1177/10298649231184920
Atroszko, P. A., Charzyńska, E., Buźniak, A., Czerwiński, S. K., Griffiths, M. D., Jankowska, A., Kamble, S., Mizik, Z., Pontes, H., Shane, J., Sussman, S., Woropay Hodziejewicz, N., & Pallesen, S. (2023b). Validity, reliability, and cross-cultural comparability of a problematic overstudying scale across European, North American, and Asian countries. International Journal of Mental Health and Addiction. Advanced online publication. https://doi.org/10.1007/s11469-023-01128-5
Atroszko, P. A., Demetrovics, Z., & Griffiths, M. D. (2020). Work addiction, obsessive-compulsive personality disorder, burn-out, and global burden of disease: Implications from the ICD-11. International Journal of Environmental Research and Public Health, 17(2), 660. https://doi.org/10.3390/ijerph17020660
Atroszko, P. A., Sawicki, A., & Kamble, S. (2019). Cross-cultural pilot study on the relationship between study addiction and narcissism among undergraduate students in Poland and India. Health Psychology Report, 7(4), 325–333. https://doi.org/10.5114/hpr.2019.88058
Bereznowski, P., & Konarski, R. (2020). Is the polythetic approach efficient in identifying potentially addicted to work individuals? Comparison of the polythetic approach with the item response theory framework. Polish Psychological Bulletin, 51(2), 98–115. https://doi.org/10.24425/ppb.2020.133768
Bereznowski, P., Atroszko, P. A., & Konarski, R. (2022). Network approach to work addiction: A cross-cultural study. PsyArXiv [Preprint]. https://doi.org/10.31234/osf.io/dy92g
Bereznowski, P., Atroszko, P. A., & Konarski, R. (2023a). Work addiction, work engagement, job burnout, and perceived stress: A network analysis. Frontiers in Psychology, 14, 1130069. https://doi.org/10.3389/fpsyg.2023.1130069
Bereznowski, P., Bereznowska, A., Atroszko, P. A., & Konarski, R. (2023b). Work addiction and work engagement: A network approach to cross-cultural data. International Journal of Mental Health and Addiction, 21(4), 2052–2076. https://doi.org/10.1007/s11469-021-00707-8
Berking, M., & Lukas, C. A. (2015). The affect regulation training (ART): A transdiagnostic approach to the prevention and treatment of mental disorders. Current Opinion in Psychology, 3, 64–69. https://doi.org/10.1016/j.copsyc.2015.02.002
Bisht, A., & Godiyal, S. (2016). Study addiction among higher secondary girls students. International Journal of Advanced Multidisciplinary Research, 3(9), 1–5. https://doi.org/10.22192/ijamr.2016.03.09.001
Borsboom, D. (2017). A network theory of mental disorders. World Psychiatry, 16(1), 5–13. https://doi.org/10.1002/wps.20375
Borsboom, D., Fried, E. I., Epskamp, S., Waldorp, L. J., van Borkulo, C. D., van der Maas, H. L. J., & Cramer, A. O. J. (2017). False alarm? A comprehensive reanalysis of “Evidence that psychopathology symptom networks have limited replicability” by Forbes, Wright, Markon, and Krueger (2017). Journal of Abnormal Psychology, 126(7), 989–999. https://doi.org/10.1037/abn0000306
Burger, J., Isvoranu, A.-M., Lunansky, G., Haslbeck, J. M. B., Epskamp, S., Hoekstra, R. H. A., Fried, E. I., Borsboom, D., & Blanken, T. F. (2022). Reporting standards for psychological network analyses in cross-sectional data. Psychological Methods. Advance online publication. https://doi.org/10.1037/met0000471
Charlton, J. P., & Danforth, I. D. W. (2007). Distinguishing addiction and high engagement in the context of online game playing. Computers in Human Behavior, 23(3), 1531–1548. https://doi.org/10.1016/j.chb.2005.07.002
Charzyńska, E., Sussman, S., & Atroszko, P. A. (2021). Profiles of potential behavioral addictions’ severity and their associations with gender, personality, and well-being: A person-centered approach. Addictive Behaviors, 119, 106941. https://doi.org/10.1016/j.addbeh.2021.106941
Clark, M. A., Michel, J. S., Zhdanova, L., Pui, S. Y., & Baltes, B. B. (2016). All work and no play? A meta-analytic examination of the correlates and outcomes of workaholism. Journal of Management, 42(7), 1836–1873. https://doi.org/10.1177/0149206314522301
Cosma, A., Stevens, G. W. J. M., Vollebergh, W. A. M., & De Looze, M. (2022). Time trends in schoolwork pressure among Dutch adolescents, 2001–2017: Gender and educational differences. Scandinavian Journal of Public Health, 50(5), 538–541. https://doi.org/10.1177/14034948211018388
Costantini, G., & Epskamp, S. (2017). EstimateGroupNetwork: Perform the joint graphical lasso and select tuning parameters. R package (Version 0.3.1) [Computer software]. Retrieved from https://cran.r-project.org/web/packages/EstimateGroupNetwork/index.html
Csardi, G., & Nepusz, T. (2006). The igraph software package for complex network research. InterJournal, 1695(5), 1–9. Retrieved from https://www.researchgate.net/publication/221995787_The_Igraph_Software_Package_for_Complex_Network_Research
Czerwiński, S. K., Lawendowski, R., Kierzkowski, M., & Atroszko, P. A. (2023). Can perseverance of effort become maladaptive? Study addiction moderates the relationship between this component of grit and well-being among music academy students. Musicae Scientiae, 27(3), 568–595. https://doi.org/10.1177/10298649221095135
De Looze, M. E., Cosma, A. P., Vollebergh, W. A. M., Duinhof, E. L., de Roos, S. A., van Dorsselaer, S., van Bon-Martens, M. J. H., Vonk, R., & Stevens, G. W. J. M. (2020). Trends over time in adolescent emotional wellbeing in the Netherlands, 2005-2017: Links with perceived schoolwork pressure, parent-adolescent communication and bullying victimization. Journal of Youth and Adolescence, 49(10), 2124–2135. https://doi.org/10.1007/s10964-020-01280-4
Epskamp, S., Borsboom, D., & Fried, E. I. (2018). Estimating psychological networks and their accuracy: A tutorial paper. Behavior Research Methods, 50(1), 195–212. https://doi.org/10.3758/s13428-017-0862-1
Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., & Borsboom, D. (2012). qgraph: Network visualizations of relationships in psychometric data. Journal of Statistical Software, 48(4), 1–18. https://doi.org/10.18637/jss.v048.i04
Fried, E. I. (2020). Lack of theory building and testing impedes progress in the factor and network literature. Psychological Inquiry, 31(4), 271–288. https://doi.org/10.1080/1047840X.2020.1853461
Forbes, M. K., Wright, A. G. C., Markon, K. E., & Krueger, R. F. (2017a). Evidence that psychopathology symptom networks have limited replicability. Journal of Abnormal Psychology, 126(7), 969–988. https://doi.org/10.1037/abn0000276
Forbes, M. K., Wright, A. G. C., Markon, K. E., & Krueger, R. F. (2017b). Further evidence that psychopathology networks have limited replicability and utility: Response to Borsboom et al. (2017) and Steinley et al. (2017). Journal of Abnormal Psychology, 126(7), 1011–1016. https://doi.org/10.1037/abn0000313
Godzwon, J. M., Wielewska, M. K., & Atroszko, P. A. (2022). The relationship of study addiction with social support and satisfaction with intimate relationships. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-022-00874-2
Griffiths, M. D. (2005). A ‘components’ model of addiction within a biopsychosocial framework. Journal of Substance Use, 10(4), 191–197. https://doi.org/10.1080/14659890500114359
Griffiths, M. D., Demetrovics, Z., & Atroszko, P. A. (2018). Ten myths about work addiction. Journal of Behavioral Addictions, 7(4), 845–857. https://doi.org/10.1556/2006.7.2018.05
Haslbeck, J. (2019). mgm: Estimating time-varying k-order mixed graphical models. R package (Version 1.2–11) [Computer software]. Retrieved from https://cran.r-project.org/web/packages/mgm/index.html
Haslbeck, J. M. B., & Waldorp, L. J. (2018). How well do network models predict observations? On the importance of predictability in network models. Behavior Research Methods, 50(2), 853–861. https://doi.org/10.3758/s13428-017-0910-x
Isvoranu, A.-M., & Epskamp, S. (2023). Which estimation method to choose in network psychometrics? Deriving guidelines for applied researchers. Psychological Methods, 28(4), 925–946. https://doi.org/10.1037/met0000439
Jouhki, H., & Oksanen, A. (2022). To get high or to get out? Examining the link between addictive behaviors and escapism. Substance Use & Misuse, 57(2), 202–211. https://doi.org/10.1080/10826084.2021.2002897
Kaggwa, M. M., Kajjimu, J., Sserunkuma, J., Najjuka, S. M., Atim, L. M., Olum, R., Tagg, A., & Bongomin, F. (2021). Prevalence of burnout among university students in low- and middle-income countries: A systematic review and meta-analysis. PloS One, 16(8), e0256402. https://doi.org/10.1371/journal.pone.0256402
Kircaburun, K., Süral, İ., March, E., Balta, S., Emirtekin, E., & Griffiths, M. D. (2021). Study addiction and ‘dark’ personality traits: A cross-sectional survey study among emerging adults. Journal of Addictive Diseases, 39(3), 307–315. https://doi.org/10.1080/10550887.2021.1872469
Klinger, D. A., Freeman, J. G., Bilz, L., Liiv, K., Ramelow, D., Sebok, S. S., Samdal, O., Dur, W., & Rasmussen, M. (2015). Cross-national trends in perceived school pressure by gender and age from 1994 to 2010. European Journal of Public Health, 25(suppl 2), 51–56. https://doi.org/10.1093/eurpub/ckv027
Kozak, S., Kaminiów, K., Biecka, A., Kuźma, K., Wyrzykowski, M., Kozłowska, M., & Brożek, G. (2020). Uzależnienie od uczenia się–rozpowszechnienie problemu wśród studentów kierunków medycznych. In Interdyscyplinarne badania z zakresu nauk pedagogicznych i humanistycznych (Vol. 107). Wydawnictwo Naukowe TYGIEL. Retrieved from http://bc.wydawnictwo-tygiel.pl/public/assets/445/Interdyscyplinarne%20badania%20z%20zakresu%20nauk%20pedagogicznych%20i%20humanistycznych.pdf
Lawendowski, R., Bereznowski, P., Wróbel, W. K., Kierzkowski, M., & Atroszko, P. A. (2020). Study addiction among musicians: Measurement, and relationship with personality, social anxiety, performance, and psychosocial functioning. Musicae Scientiae, 24(4), 449–474. https://doi.org/10.1177/1029864918822138
Loscalzo, Y., & Giannini, M. (2018a). Problematic overstudying: Studyholism or study addiction?: Commentary on: Ten myths about work addiction (Griffiths et al., 2018). Journal of Behavioral Addictions, 7(4), 867–870. https://doi.org/10.1556/2006.7.2018.124
Loscalzo, Y., & Giannini, M. (2018b). The Bergen Study Addiction Scale: Psychometric properties of the Italian version. A pilot study. Psychiatria i Psychologia Kliniczna, 18(3), 271–275. https://doi.org/10.15557/PiPK.2018.0033
Moskalewicz, J., Badora, B., Feliksiak, M., Głowacki, A., Gwiazda, M., Herrmann, M., Kawalec, I., & Roguska, B. (2019). Oszacowanie rozpowszechnienia oraz identyfikacja czynników ryzyka i czynników chroniących hazardu i innych uzależnień behawioralnych–edycja 2018/2019. Polish Ministry of Health. Retrieved from https://www.kbpn.gov.pl/portal?id=15&res_id=9249205
Nerstad, C. G. L., Richardsen, A. M., & Martinussen, M. (2010). Factorial validity of the Utrecht Work Engagement Scale (UWES) across occupational groups in Norway. Scandinavian Journal of Psychology, 51(4), 326–333. https://doi.org/10.1111/j.1467-9450.2009.00770.x
Pascoe, M. C., Hetrick, S. E., & Parker, A. G. (2020). The impact of stress on students in secondary school and higher education. International Journal of Adolescence and Youth, 25(1), 104–112. https://doi.org/10.1080/02673843.2019.1596823
Pollak, A., Chrupała-Pniak, M., Rudnicka, P., & Paliga, M. (2017). Work engagement—A systematic review of Polish research. Polish Psychological Bulletin, 48(2), 175–187. https://doi.org/10.1515/ppb-2017-0021
R Core Team. (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Retrieved from https://www.R-project.org
Robinson, B. E. (2014). Chained to the desk: A guidebook for workaholics, their partners and children, and the clinicians who treat them. New York University Press.
Schaufeli, W., & Bakker, A. (2004). UWES: Utrecht Work Engagement Scale. Preliminary Manual. Occupational Health Psychology Unit, Utrecht University.
Schaufeli, W. B., Bakker, A. B., & Salanova, M. (2006). The measurement of work engagement with a short questionnaire: A cross-national study. Educational and Psychological Measurement, 66(4), 701–716. https://doi.org/10.1177/0013164405282471
Schaefer, J., & Strob, J. (2023). Wenn das Studieren außer Kontrolle gerät. Zeitschrift Fur Klinische Psychologie Und Psychotherapie, 52(1), 25–37. https://doi.org/10.1026/1616-3443/a000684
Sussman, S., & Sussman, A. N. (2011). Considering the definition of addiction. International Journal of Environmental Research and Public Health, 8(10), 4025–4038. https://doi.org/10.3390/ijerph8104025
Sussman, S. (2012). Workaholism: A review. Journal of Addiction Research and Theory, S6. 10.4172/2155-6105.S6–001
van Borkulo, C., Boschloo, L., Kossakowski, J. J., Tio, P., Schoevers, R. A., Brosboom, D., & Waldorp, L. J. (2017). Comparing network structures on three aspects: A permutation test. Unpublished manuscript. https://doi.org/10.13140/RG.2.2.29455.38569
Vijayakumar, N., de Macks, Z. O., Shirtcliff, E. A., & Pfeifer, J. H. (2018). Puberty and the human brain: Insights into adolescent development. Neuroscience & Biobehavioral Reviews, 92, 417–436. https://doi.org/10.1016/j.neubiorev.2018.06.004
Walburg, V. (2014). Burnout among high school students: A literature review. Children and Youth Services Review, 42, 28–33. https://doi.org/10.1016/j.childyouth.2014.03.020
World Health Organization (2019). International statistical classification of diseases and related health problems, 11th Revision. https://icd.who.int/en.
Woropay-Hordziejewicz, N. A., Buźniak, A., Lawendowski, R., & Atroszko, P. A. (2022). Compulsive study behaviors are associated with eating disorders and have independent negative effects on well-being: A structural equation model study among young musicians. Sustainability, 14, 8617. https://doi.org/10.3390/su14148617
Wróbel, W. K. (2020). Study addiction among high school students: Measurement and relationship with psychopathology, personality, quality of life, and school variables (Unpublished Master's thesis). University of Gdańsk.
Code Availability
The analytic code for all analyses performed in this study is available at https://osf.io/f5vsq/?view_only=ab6f0e77ce054c759fca0506a2ffe5bf.
Funding
This work was supported by the Ministry of Science and Higher Education under Grant “Diamentowy Grant” DI 2017 001247.
Author information
Authors and Affiliations
Contributions
PB assisted with obtaining funding, literature search, study design and concept, statistical analyses, data interpretation, generation of the initial draft of the manuscript, and final editing and approval of the manuscript. RK assisted with study design and concept and final editing and approval of the manuscript. SP assisted with data collection and final editing and approval of the manuscript. PAA assisted with literature search, study design and concept, data collection, data interpretation, generation of the initial draft of the manuscript, and final editing and approval of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent
The study was carried out in accordance with the Declaration of Helsinki. All gathered data was anonymous, and participants were informed about all the proper details about the study and their role in it, including that they can withdraw at any point. Attaining formal and written informed consent was not regarded as necessary as voluntary completion of the questionnaires was regarded as providing consent, and no medical information was gathered. The study was approved by the Norwegian Data Protection Official for Research and the Research Ethics Committee at the Institute of Psychology of the University of Gdańsk in Poland.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bereznowski, P., Konarski, R., Pallesen, S. et al. Similarities and Differences Between Study Addiction and Study Engagement and Work Addiction and Work Engagement: A Network Analysis. Int J Ment Health Addiction (2024). https://doi.org/10.1007/s11469-023-01234-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-023-01234-4