
Abstract
Purpose
Sex-steroid hormones are associated with postmenopausal breast cancer but potential confounding from other biological pathways is rarely considered. We estimated risk ratios for sex-steroid hormone biomarkers in relation to postmenopausal estrogen receptor (ER)-positive breast cancer, while accounting for biomarkers from insulin/insulin-like growth factor-signaling and inflammatory pathways.
Methods
This analysis included 1208 women from a case–cohort study of postmenopausal breast cancer within the Melbourne Collaborative Cohort Study. Weighted Poisson regression with a robust variance estimator was used to estimate risk ratios (RRs) and 95% confidence intervals (CIs) of postmenopausal ER-positive breast cancer, per doubling plasma concentration of progesterone, estrogens, androgens, and sex-hormone binding globulin (SHBG). Analyses included sociodemographic and lifestyle confounders, and other biomarkers identified as potential confounders.
Results
Increased risks of postmenopausal ER-positive breast cancer were observed per doubling plasma concentration of progesterone (RR: 1.22, 95% CI 1.03 to 1.44), androstenedione (RR 1.20, 95% CI 0.99 to 1.45), dehydroepiandrosterone (RR: 1.15, 95% CI 1.00 to 1.34), total testosterone (RR: 1.11, 95% CI 0.96 to 1.29), free testosterone (RR: 1.12, 95% CI 0.98 to 1.28), estrone (RR 1.21, 95% CI 0.99 to 1.48), total estradiol (RR 1.19, 95% CI 1.02 to 1.39) and free estradiol (RR 1.22, 95% CI 1.05 to 1.41). A possible decreased risk was observed for SHBG (RR 0.83, 95% CI 0.66 to 1.05).
Conclusion
Progesterone, estrogens and androgens likely increase postmenopausal ER-positive breast cancer risk, whereas SHBG may decrease risk. These findings strengthen the causal evidence surrounding the sex-hormone-driven nature of postmenopausal breast cancer.
Similar content being viewed by others


Background
Breast cancer is a largely hormone-driven disease and the relationships between endogenous sex-steroid hormones – especially estrogens – and postmenopausal breast cancer are thought to be well established [1,2,3]. A recent systematic review and meta-analysis found moderate- to high-quality evidence that higher levels of estrogens and androgens, and lower levels of sex-hormone binding globulin (SHBG), were associated with increased risks of postmenopausal breast cancer [4]. The quality of the evidence in this review was largely determined by dose–response effects and large effect sizes [4]. No extracted result had adjusted for biomarkers from other biological pathways; namely, the insulin/insulin-like growth factor (IGF)-signaling and inflammatory pathways. These pathways may confound the effect of the sex-steroid hormone pathway (Fig. 1). For example, insulin and insulin-like growth factor-1 (IGF-1) can affect the bioavailability of estrogens and androgens via the regulation of aromatase and suppression of hepatic SHBG production [1, 5, 6]. They may also play a role in breast carcinogenesis: insulin and the IGF axis are proposed to have mitogenic and anti-apoptotic properties, and higher systemic concentrations of IGF-1 are associated with increased risks of breast cancer [1, 2, 5,6,7,8]. Further, a state of low-grade chronic inflammation – for example, in the context of physical inactivity and obesity – can foster a pro-carcinogenic environment via the overstimulation and dysregulation of immune cells, cytokines and adipokines [1, 2, 5, 6, 9]. Higher circulating levels of C-reactive protein (CRP) – a non-specific marker of chronic inflammation – are associated with increased risks of breast cancer, but the epidemiological evidence for other inflammatory markers remains uncertain [2, 10, 11]. Higher circulating levels of pro-inflammatory biomarkers including leptin, tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) are also associated with enhanced aromatase activity and lower circulating levels of SHBG [1, 2, 5, 6, 9, 12].

Diagram of the assumed interrelationships between the inflammatory, insulin/insulin-like growth factor-signaling, and sex-steroid hormone pathways. SHBG sex-hormone binding globulin, CRP C-reactive protein, IGF insulin-like growth factor, IGF-1 Insulin-like growth factor-1
The aim of this study was to estimate risk ratios for sex-steroid hormone biomarkers in relation to postmenopausal breast cancer in a case-cohort of postmenopausal women within the Melbourne Collaborative Cohort Study (MCCS), while accounting for other biomarkers from the insulin/IGF-signaling and inflammatory pathways.
Methods
The Melbourne Collaborative Cohort Study
The MCCS includes 24,469 women aged 40–69 at recruitment from 1990 to 1994 [13]. At baseline and the second follow-up (F2, 2003–7), participants provided information about health status, lifestyle factors, sociodemographics and medical history via structured questionnaires [13]. Anthropometric and clinical measurements were performed at the study center, including the collection of blood samples [13]. At both times, plasma was stored in liquid nitrogen. Data linkages to national and state death and cancer registries—including the Victorian Cancer Registry and Australian Cancer Database—enabled vital status and cancer diagnoses to be determined prospectively [13]. The study protocol was approved by the Cancer Council Victoria Human Research Ethics Committee.
The case-cohort study
Initial eligibility criteria at second follow-up (2003–7)
This case-cohort study was restricted to women who attended F2. At F2, eligible women were postmenopausal, not known to be taking hormone replacement therapy (HRT), had provided a blood sample (within one year of the F2 questionnaire, if completed), had no prior invasive cancer diagnosis (except for keratinocyte cancers); at baseline, they had a body mass index (BMI) ≥ 18.5 kg/m2. Women were considered postmenopausal if they had had no menstrual periods in the past 12 months and met one of the following criteria: had experienced natural cessation of menses; had a bilateral oophorectomy; were age 55 years or older; or had had no periods in the 12 months prior to baseline and, for participants in a previous case-cohort study, measured estradiol concentration below 109 pmol/L at baseline (a threshold from that study [14, 15]). The case-cohort comprised a random sample of the 10,669 eligible women and all eligible women diagnosed with estrogen receptor (ER)-positive postmenopausal breast cancer between blood collection at F2 and 31 October 2020.
An eligible tumor was defined as invasive adenocarcinoma of the breast (International Classification of Diseases, Tenth Revision [ICD-10] code C50) that was ER-positive. Tumors of unknown hormone receptor status were included as 88% of breast cancer diagnoses among eligible women of known ER status were ER-positive. ER-negative and progesterone receptor (PR)-positive cancers were also included as this tumor subtype may be misclassified and accounts for only 1–4% of diagnoses [16,17,18,19]. Unspecified adenocarcinomas and unspecified cancers were presumed to be adenocarcinomas as 99% of breast cancer diagnoses among eligible women of known morphology were adenocarcinomas.
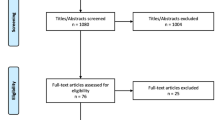
In total, 1,412 women were selected for the case-cohort study, including 999 in the subcohort and 459 cases (46 from the subcohort) (Fig. 2). The subcohort was a random sample of eligible women (Online Resource 1).

Selection of participants into the case-cohort study and analyses. N Number, F2 second follow-up wave, HRT hormone replacement therapy, BMI body mass index (kg/m.2)
Post-hoc criteria
Of the 1,412 selected women, 286 (20%) had unknown menopausal status and/or HRT use. Eligibility was confirmed for all selected women using the distribution of measured estradiol values at F2 for naturally postmenopausal women who were not taking HRT (806, 57% of selected women). Thirty-two women with estradiol values at or above the 99th percentile of this distribution (29.3 pg/mL, equivalent to 107.6 pmol/L) were excluded, regardless of age, menopausal status, or HRT use. Menopausal status and/or HRT use could not be determined for six women missing estradiol measurements. One woman was excluded as she did not participate in F2 despite providing a blood sample.
Four cases outside the subcohort were retrospectively disqualified as cases; three diagnoses were ascertained from death certificate only and one woman was diagnosed with non-adenocarcinoma breast cancer. To minimize the impact of death as a competing risk, follow-up was chosen to end on participants’ 86th birthday (Online Resource 2). Thus, 44 cases outside the subcohort were excluded and eight cases within the subcohort were analyzed as non-cases. Thirteen users of exogenous insulin were excluded so that measured insulin concentrations were of endogenous insulin.
The total study sample after post-hoc exclusions comprised 1,312 women, 969 in the subcohort and 378 cases (35 also in the subcohort) (Fig. 2).
Laboratory analysis of plasma biomarkers
Plasma samples of selected women were randomly ordered and allocated into 21 batches containing approximately equal numbers of cases. The samples were shipped on dry ice in two dispatches to the International Agency for Research on Cancer (IARC).
The plasma concentrations of all biomarkers were measured at the Nutrition Metabolism Branch, IARC. Plasma concentrations of sex-steroid hormones and SHBG were measured as previously described [20]. In brief, sex-steroid hormone concentrations were measured using a liquid chromatography-mass spectrometry system consisting of an ultra-high-performance liquid chromatograph (Agilent 1290, Agilent, Santa Clara, CA) and a QTRAP 5500 mass spectrometer (SCIEX, Framingham, MA). SHBG concentrations were measured by solid-phase “sandwich” enzyme-linked immunoassay (DRG International, Springfield, NJ). Interferon gamma (IFN-γ), IL-6, interleukin-8 (IL-8), interleukin-10 (IL-10), TNF-α, insulin, adiponectin, leptin, and CRP were measured by highly-sensitive and highly-specific electrochemiluminescent methods (Meso Scale Discovery, Rockville, MD). IGF-1 and insulin-like growth factor binding protein-3 (IGFBP-3) were measured by immunoassay methods by R&D Systems (Biotechne, Minneapolis, USA). C-peptide was measured by an enzyme-linked immunosorbent assay by ALPCO (Salem, USA). Further details are included in Online Resource 3. Three quality control samples at different concentration levels were measured in duplicate in each batch of analyses to assess the reliability of biomarker measurements. Reliability was assessed by calculating intra-assay and inter-assay coefficients of variation (CVs), as well as intra-batch and inter-batch intra-class correlation coefficients (ICCs), as described in Online Resource 4. Assay performance for estradiol and testosterone was evaluated by measuring samples created from reference standards with known concentrations. Measured values were compared with true values using validity coefficients and correlation plots, as described in Online Resource 5.
Normalization of biomarker values
Biomarker data were cleaned and normalized to correct for effects of batch, dispatch, and time since last meal (12% of study participants were not fasting at blood collection). The normalization technique was adapted from Viallon et al. [21]. Normalization models were used to estimate residual ICCs for the total proportion of variation attributable to batch for each biomarker. Methods for normalization and estimated ICCs are presented in Online Resource 6.
Calculation of free estradiol and free testosterone
Concentrations of free estradiol and free testosterone (i.e., not bound to SHBG) were calculated from normalized values of estradiol, testosterone and SHBG using the law of mass action assuming a fixed albumin concentration of 40 g/L (5.97 × 10–4 mol/L) and the following association constants: 6 × 104 L/mol (binding of estradiol to albumin); 4 × 104 L/mol (binding of testosterone to albumin); 0.68 × 109 L/mol (binding of estradiol to SHBG); 1.6 × 109 L/mol (binding of testosterone to SHBG) [22,23,24,25].
Statistical analysis
Descriptive statistics were presented as medians and interquartile ranges (IQRs) or as frequencies and percentages, where appropriate. Weighted modified Poisson regression with a robust variance estimator was used to estimate risk ratios (RRs) and 95% confidence intervals (CIs) of postmenopausal ER-positive breast cancer, per doubling plasma concentration of progesterone, androstenedione, DHEA, total and calculated free testosterone, estrone, total and calculated free estradiol, and SHBG. Poisson regression models were weighted to account for the oversampling of cases, which can be considered a stratified form of sampling in which stratification depends on the outcome [26]. Case weights were one, and weights for non-cases were the inverse of the sampling probability for non-cases [26]. The latter was calculated as the number of non-cases in the eligible cohort divided by the number of non-cases in the subcohort ([10,669—459] /953).
Confounders including other biomarkers were identified a priori using causal diagrams informed by expert consensus and literature review. Sociodemographic and lifestyle confounders included: education; country of birth; socioeconomic disadvantage; diet at baseline (dietary intake of carotenoids and dietary intake of calcium); alcohol consumption at baseline; smoking status at baseline; adiposity at baseline; physical activity at F2; age at blood collection; and age at menopause. The identification, measurement and modelling of sociodemographic and lifestyle confounders are described in Online Resource 7. As age at menopause could only be measured for naturally postmenopausal women (821, 63% of the case-cohort after post-hoc exclusions), this variable was not included in the adjustment set for the primary analyses. Sensitivity analyses were conducted, restricting to naturally postmenopausal women with a recorded age at menopause to include this variable in adjustment sets. Biomarkers that were identified as potential confounders a priori but had correlations ≥ 0.50 with the biomarker of interest were not included in the primary analysis (Online Resource 8).
The primary analyses modelled all biomarker concentrations as continuous, normalized values on the log2-scale. A one unit increase on the log2-scale represents a doubling in biomarker concentration. Analyses were repeated without adjustment for other biomarkers (where applicable). Sensitivity analyses excluding ER-negative/PR-positive tumors and tumors of unknown hormone receptor status were conducted to test the assumption that these tumor subtypes were ER-positive. Additional sensitivity analyses excluded all cases diagnosed within one year of blood draw at F2 to assess the potential impact of reverse causation. These analyses also excluded deaths that occurred within this time frame to be consistent with the target trial approach [27]. In addition, analyses that modelled concentrations of each sex-steroid hormone biomarker as quartiles corresponding to the distribution of normalized biomarker values in the subcohort were performed without adjustment for other biomarkers.
All analyses were complete-case analyses. The linearity assumption was tested for the continuous, normalized biomarker values using restricted cubic splines and Wald-tests. All statistical analyses were performed using Stata 16 (StataCorp, College Station, TX).
Results
Of the 1312 women eligible after post-hoc exclusions, 87 were excluded due to missing sociodemographic and lifestyle confounder data (Fig. 2). In addition, 17 women were excluded due to missing measurements for all sex-steroid hormone biomarkers. The characteristics of the remaining 1,208 women are summarized in Table 1. Compared with non-cases, cases were more likely to be educated, have obesity, and experience the menopause at ≥ 53 years, and were less likely to be sufficiently active. The normalized concentrations of DHEA, total estradiol, free estradiol, leptin and CRP were higher, and the normalized concentration of SHBG was lower, for cases compared with non-cases. The characteristics of the 1,312 women eligible after post-hoc exclusions were not appreciably different from the 1,208 women analyzed (Online Resource 9).
Of the 342 cases eligible for complete-case analysis, 324 (95%) were ER-positive, 5 were ER-negative/PR-positive, and 13 were of unknown hormone receptor status. Twenty cases were diagnosed within one year of blood draw at F2, and 5 subcohort non-cases had died.
Reliability of biomarker measurements and assay performance
The calculated overall intra-assay and inter-assay CVs were below 10% and 15%, respectively, for most biomarkers (Online Resource Table 4.1). The estimated intra-batch and inter-batch reliability ICCs were above 80% and 70%, respectively, for most biomarkers (Online Resource Table 4.2). The validity coefficients for the true and measured values of estradiol and testosterone were 0.987 and 0.997, respectively. Correlation plots are presented in Online Resource 5.
Risk ratios per doubling of biomarker concentration
For the primary analyses, increased risks of postmenopausal ER-positive breast cancer were observed per doubling plasma concentration of progesterone (RR 1.22, 95% CI 1.03 to 1.44), androstenedione (RR 1.20, 95% CI 0.99 to 1.45), DHEA (RR 1.15, 95% CI 1.00 to 1.34), total testosterone (RR 1.11, 95% CI 0.96 to 1.29), calculated free testosterone (RR: 1.12, 95% CI: 0.98 to 1.28), estrone (RR: 1.21, 95% CI: 0.99 to 1.48), total estradiol (RR: 1.19, 95% CI: 1.02 to 1.39) and calculated free estradiol (RR: 1.22, 95% CI: 1.05 to 1.41) (Table 2). A decreased risk was suggested for SHBG (RR: 0.83, 95% CI: 0.66 to 1.05).
Results did not appreciably differ in analyses without adjustment for other biomarkers (Table 2), except that the inverse association for SHBG was somewhat weaker (RR: 0.90, 95% CI: 0.73 to 1.11). Point estimates for RR for all sex-steroid hormone biomarkers were slightly stronger when ER-negative/PR-positive tumors and tumors of unknown hormone receptor status were excluded (Online Resource 10). The results of the sensitivity analyses excluding cases and deaths that occurred within one year of blood draw at F2 were similar to the results of the primary analyses (Online Resource 11).
For the sensitivity analyses in the subset of naturally postmenopausal women with a recorded age at menopause (Online Resource 12), the point estimates for RR were closer to the null for progesterone (RR 1.11, 95% CI 0.90 to 1.36) and androstenedione (RR 1.08, 95% CI 0.85 to 1.39), and further away from the null for estrone (RR 1.30, 95% CI 0.99 to 1.69), total estradiol (RR 1.29, 95% CI 1.04 to 1.58) and calculated free estradiol (RR 1.31, 95% CI 1.08 to 1.60). Results with and without adjustment for age at menopause were similar, whereas the point estimates for RR without adjustment for other biomarkers were closer to the null for estrone, free estradiol and SHBG (Online Resource 12).
Risk ratios for quartiles of biomarker concentration
The highest versus lowest levels of biomarker concentrations were associated with increased risks of postmenopausal ER-positive breast cancer for progesterone (RR 1.56, 95% CI 1.09 to 2.24), androstenedione (RR 1.39, 95% CI 0.97 to 2.00), DHEA (RR 1.55, 95% CI 1.06 to 2.25), total estradiol (RR 1.49, 95% CI 1.01 to 2.19) and calculated free estradiol (RR 1.47, 95% CI 0.99 to 2.17) (Table 3). RRs were suggestive of monotonic increases for DHEA, estrone and total estradiol. In contrast, the positive relationship between calculated free estradiol and postmenopausal ER-positive breast cancer plateaued at the third-highest plasma concentration compared to the lowest.
Discussion
Summary of principal findings
Higher plasma concentrations of progesterone, estrogens and androgens, and decreasing plasma concentration of SHBG, were associated with increased risks of postmenopausal ER-positive breast cancer in this case-cohort of postmenopausal women. Similar results were obtained with and without control for other biomarkers that were identified as potential confounders, suggesting that confounding by the insulin/IGF-signaling and inflammatory pathways was minimal. The exception was SHBG; a somewhat stronger inverse relationship was observed with adjustment for adiponectin, leptin, insulin and IGF-1. Slightly stronger associations were observed when cases that were ER-negative/PR-positive or of unknown hormone receptor status were excluded, indicating that some cases that were assumed to be ER-positive may not have truly been ER-positive. The impact of reverse causation was negligible. Results of the sensitivity analyses in the subset of naturally postmenopausal women with a recorded age at menopause were not sensitive to adjustment for age at menopause. Rather, the deviations observed from the primary analyses could be explained by reduced precision in the subsample, or differences between women who were naturally postmenopausal (with a known age at menopause) and women who were assumed to be postmenopausal for other reasons.
Strengths and limitations
A strength of our study was that careful consideration was given to biomarkers from the insulin/IGF-signaling and inflammatory pathways that may confound the associations between biomarkers of the sex-steroid hormone pathway and risk of postmenopausal ER-positive breast cancer. Biomarkers that may be potential confounders were identified a priori using a causal diagram that was informed by literature review and expert opinion. Causal diagrams can minimize the pitfalls of other confounder selection methods, including overadjustment bias [28,29,30]. However, residual confounding may remain if our assumptions are inaccurate or if important confounders have not been identified or correctly measured [28, 30]. Depicting the true complexity of biomarker interrelationships and their role in breast carcinogenesis is challenging. The current body of causal knowledge is limited, and we could not account for bidirectional relationships as the biomarkers had only been measured at one point in time. Thus, we assumed what the net direction of the effects of the measured biomarkers would be in a relatively older cohort of postmenopausal women in our causal diagram. Our assumptions can be refined with the advancement of causal knowledge over time, ideally in studies that measure biomarkers at multiple points in time.
A potential limitation of our study was that selection bias may have been introduced if there were systematic differences between women who did and did not attend F2 and provide a blood sample. However, the sociodemographic and lifestyle confounders that we have adjusted for in our analyses are likely to have included the critical determinants of participation at F2 (e.g., age, country of birth, socioeconomic disadvantage, education, smoking, alcohol, adiposity) [13]. Restriction to women who had not been diagnosed with breast cancer before F2 could potentially bias the RR for hormones towards the null, since women with high hormone concentrations at baseline were more likely to develop breast cancer [15]. Bias may also arise due to the exclusion of participants with missing data, although in this study, the proportion of eligible women with missing data was small (8%). Considered collectively, we expect selection bias to have minimal impact on our study conclusions. We note that our findings are only generalizable to postmenopausal women who are not taking hormone replacement therapy or exogenous insulin and have no personal history of cancer (including breast cancer).
A major strength of our study was the use of a highly sensitive liquid chromatography-mass spectrometry method to measure the plasma concentrations of sex-steroid hormones in postmenopausal women with high precision and accuracy. We were able to demonstrate the validity of this method using reference standards for estradiol and testosterone. The measured and true values of estradiol and testosterone were highly correlated. Further, intra-assay and inter-assay CVs, as well as intra-batch and inter-batch ICCs, calculated from quality control samples indicated that biomarker measurements were reliable, with few exceptions that may be attributable to batch and dispatch effects (Online Resource 4). We adopted a novel analysis approach to correct for batch effects, dispatch effects and time since last meal, whilst retaining meaningful biological variation in the biomarker measurements [21]. Further, we measured the plasma concentrations of a breadth of biomarkers from the inflammation, insulin/IGF-signaling and sex-steroid hormone pathways, which were selected through expert consultation and literature review. However, plasma concentrations of biomarkers measured at only one point in time will not be perfect proxies of complex and time-varying biological processes that may operate at cellular and systemic levels.
Comparison with other studies
Previous studies that have adjusted for other biomarkers have typically compared results with and without adjustment for other sex-steroid hormones and/or SHBG [3, 15, 31,32,33,34,35,36,37,38,39]. These are often mutual or progressive adjustments to assess “independence” rather than confounding, on the basis that biomarkers share complex interrelationships and correlations. However, this practice can lead to overadjustment bias, which we have attempted to minimize by explicitly considering our assumed underlying causal structure a priori [29]. In addition, only a handful of other studies have measured and adjusted for biomarkers from other biological pathways that may be potential confounders. One study from the Women’s Health Initiative presented results for estradiol with and without adjustment for free IGF-1 and insulin; positive associations with postmenopausal breast cancer appeared stronger with adjustment for both IGF-1 and insulin [40]. In contrast, our results for estradiol were similar with and without adjustment for biomarkers that were identified as potential confounders (adiponectin, leptin, TNF-α, IL-6, IGF-1, insulin and SHBG). Another study from the UK Biobank presented results for total testosterone with and without adjustment for SHBG and IGF-1 that were not appreciably different [41]. Likewise, our results for total testosterone did not change with and without adjustment for SHBG, but IGF-1 was not identified as a potential confounder of this analysis.
Overall, our findings were generally consistent with previous studies, including a recent systematic review by Drummond et al. [4], a previous case-cohort study conducted at baseline (1990–1994) within the MCCS [15], and a pooled analysis of nine prospective studies examining the relationship between endogenous sex-steroid hormones and postmenopausal breast cancer [3]. A notable finding was the estimated risk ratio per doubling plasma concentration of progesterone; we observed the largest increased risk of postmenopausal ER-positive breast cancer for this biomarker (RR 1.22, 95% CI 1.03 to 1.44) compared to any other measured biomarker from the sex-steroid hormone pathway. Previous studies have either not measured endogenous progesterone or have drawn inconclusive results regarding its relationship with breast cancer after the menopause, largely due to insufficient assay sensitivity and low circulating levels in postmenopausal women [42]. Our result is in support of a recent study by Trabert et al. [43], which also used a highly sensitive liquid chromatography-mass spectrometry method and found increased risks of postmenopausal breast cancer per standard deviation increase in circulating endogenous progesterone levels (hazard ratio for invasive breast cancers: 1.24, 95% CI 1.07 to 1.43). Trabert et al. [43] also present evidence for effect modification: reduced risks of postmenopausal breast cancer were observed with higher levels of progesterone among women in the lowest quintile of circulating estradiol (< 6.30 pg/mL), while increased risks were observed among women in the higher quintiles (≥ 6.30 pg/mL). Collectively, these results may challenge the plausibility of our a priori assumption that progesterone does not have a direct effect on postmenopausal ER-positive breast cancer (depicted by no direct arrow from progesterone to postmenopausal breast cancer in our causal diagram, Online Resource Fig. 8.1). This assumption was based on the systematic review by Drummond et al. [4], which found moderate quality evidence of no association between progesterone and breast cancer risk (albeit in both pre- and postmenopausal women combined). The implication of this assumption is that we should interpret the risk ratio for progesterone as an indirect effect, possibly driven by its role as a precursor of androgens and estrogens in steroidogenesis. This finding—in addition to concerns over the sensitivity of progesterone measurements in early studies, as well as studies demonstrating paracrine effects of progesterone via neighboring PR-positive cells [42]—warrants future studies including mediation analyses to determine what dictates the effect of progesterone on postmenopausal ER-positive breast cancer.
Implications and future directions
Our study confirms the causal role that sex-steroid hormones and SHBG play in the etiology of postmenopausal ER-positive breast cancer. We strengthen the causal evidence by demonstrating that potential confounding from other biological pathways implicated in breast carcinogenesis is likely non-substantial. However, the limited state of causal knowledge about biomarker interrelationships and the potential for residual confounding should be considered when interpreting our findings. Of note, two recent systematic reviews found insufficient evidence to establish a causal link between the inflammation and insulin/IGF-signaling pathways and breast cancer [8, 11]. Future research could examine whether adjustment for biomarkers from other biological pathways is more important for pre–menopausal breast cancer or ER-negative postmenopausal breast cancer. In addition, time-varying confounding could be examined in future studies that measure biomarkers at multiple points in time.
Data availability
The dataset generated for the current study is not publicly available due to compliance with participant informed consent and human research ethics committee approvals, but can be requested by contacting pedigree@cancervic.org.au.
References
Gérard C, Brown KA (2018) Obesity and breast cancer - Role of estrogens and the molecular underpinnings of aromatase regulation in breast adipose tissue. Mol Cell Endocrinol 466:15–30. https://doi.org/10.1016/j.mce.2017.09.014
(2018) Absence of Excess Body Fatness. IARC Handbooks of Cancer Prevention. IARC, Lyon
Key T, Appleby P, Barnes I, Reeves G (2002) Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J Natl Cancer Inst 94:606–616. https://doi.org/10.1093/jnci/94.8.606
Drummond AE, Swain CTV, Brown KA et al (2022) Linking physical activity to breast cancer via sex steroid hormones, Part 2: the effect of sex steroid hormones on breast cancer risk. Cancer Epidemiol Biomarkers Prev 31:28–37. https://doi.org/10.1158/1055-9965.Epi-21-0438
Friedenreich CM, Ryder-Burbidge C, McNeil J (2021) Physical activity, obesity and sedentary behavior in cancer etiology: epidemiologic evidence and biologic mechanisms. Mol Oncol 15:790–800. https://doi.org/10.1002/1878-0261.12772
Lynch BM, Leitzmann MF (2017) An evaluation of the evidence relating to physical inactivity, sedentary behavior, and cancer incidence and mortality. Current Epidemiol Rep 4:221–231. https://doi.org/10.1007/s40471-017-0119-7
Key TJ, Appleby PN, Reeves GK, Roddam AW (2010) Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: pooled individual data analysis of 17 prospective studies. Lancet Oncol 11:530–542. https://doi.org/10.1016/s1470-2045(10)70095-4
Drummond AE, Swain CTV, Milne RL et al (2022) Linking physical activity to breast cancer risk via the insulin/insulin-like growth factor signaling system, Part 2: the effect of insulin/insulin-like growth factor signaling on breast cancer risk. Cancer Epidemiol Biomarkers Prev 31:2116–2125. https://doi.org/10.1158/1055-9965.Epi-22-0505
Sánchez-Jiménez F, Pérez-Pérez A, de la Cruz-Merino L, Sánchez-Margalet V (2019) Obesity and breast cancer: role of leptin. Front Oncol 9:596. https://doi.org/10.3389/fonc.2019.00596
Chan DS, Bandera EV, Greenwood DC, Norat T (2015) Circulating C-reactive protein and breast cancer risk-systematic literature review and meta-analysis of prospective cohort studies. Cancer Epidemiol Biomarkers Prev 24:1439–1449. https://doi.org/10.1158/1055-9965.Epi-15-0324
Lou MWC, Drummond AE, Swain CTV et al (2023) Linking physical activity to breast cancer via inflammation, Part 2: the effect of inflammation on breast cancer risk. Cancer Epidemiol Biomarkers Prev 32:597–605. https://doi.org/10.1158/1055-9965.Epi-22-0929
Simó R, Sáez-López C, Barbosa-Desongles A, Hernández C, Selva DM (2015) Novel insights in SHBG regulation and clinical implications. Trends Endocrinol Metab 26:376–383. https://doi.org/10.1016/j.tem.2015.05.001
Milne RL, Fletcher AS, MacInnis RJ et al (2017) Cohort profile: the melbourne collaborative cohort study (Health 2020). Int J Epidemiol 46:1757–i. https://doi.org/10.1093/ije/dyx085
Baglietto L, English DR, Hopper JL et al (2009) Circulating steroid hormone concentrations in postmenopausal women in relation to body size and composition. Breast Cancer Res Treat 115:171–9. https://doi.org/10.1007/s10549-008-0069-3
Baglietto L, Severi G, English DR et al (2010) Circulating steroid hormone levels and risk of breast cancer for postmenopausal women. Cancer Epidemiol Biomarkers Prev 19:492–502. https://doi.org/10.1158/1055-9965.Epi-09-0532
Hefti MM, Hu R, Knoblauch NW et al (2013) Estrogen receptor negative/progesterone receptor positive breast cancer is not a reproducible subtype. Breast Cancer Res 15:R68. https://doi.org/10.1186/bcr3462
Olivotto IA, Truong PT, Speers CH et al (2004) Time to stop progesterone receptor testing in breast cancer management. J Clin Oncol 22:1769–70. https://doi.org/10.1200/jco.2004.99.251
De Maeyer L, Van Limbergen E, De Nys K et al (2008) Does estrogen receptor negative/progesterone receptor positive breast carcinoma exist? J Clin Oncol 26(335–6):5. https://doi.org/10.1200/jco.2007.14.8411
Nadji M, Gomez-Fernandez C, Ganjei-Azar P, Morales AR (2005) Immunohistochemistry of estrogen and progesterone receptors reconsidered: experience with 5993 breast cancers. Am J Clin Pathol 123:21–7. https://doi.org/10.1309/4wv79n2ghj3x1841
Mori N, Keski-Rahkonen P, Gicquiau A et al (2021) Endogenous circulating sex hormone concentrations and colon cancer risk in postmenopausal women: a prospective study and meta-analysis. JNCI Cancer Spectr. https://doi.org/10.1093/jncics/pkab084
Viallon V, His M, Rinaldi S et al (2021) A new pipeline for the normalization and pooling of metabolomics data. Metabolites 11:631. https://doi.org/10.3390/metabo11090631
Endogenous Hormones and Breast Cancer Collaborative Group (2003) Free estradiol and breast cancer risk in postmenopausal women: comparison of measured and calculated values. Cancer Epidemiol Biomark Prev 12:1457–61
Dunn JF, Nisula BC, Rodbard D (1981) Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. J Clin Endocrinol Metab 53:58–68. https://doi.org/10.1210/jcem-53-1-58
Rinaldi S, Geay A, Déchaud H et al (2002) Validity of free testosterone and free estradiol determinations in serum samples from postmenopausal women by theoretical calculations. Cancer Epidemiol Biomarkers Prev 11:1065–71
Södergård R, Bäckström T, Shanbhag V, Carstensen H (1982) Calculation of free and bound fractions of testosterone and estradiol-17 beta to human plasma proteins at body temperature. J Steroid Biochem 16:801–10. https://doi.org/10.1016/0022-4731(82)90038-3
Borgan O, Langholz B, Samuelsen SO, Goldstein L, Pogoda J (2000) Exposure stratified case-cohort designs. Lifetime Data Anal 6:39–58. https://doi.org/10.1023/a:1009661900674
Hernán MA, Sauer BC, Hernández-Díaz S, Platt R, Shrier I (2016) Specifying a target trial prevents immortal time bias and other self-inflicted injuries in observational analyses. J Clin Epidemiol 79:70–5. https://doi.org/10.1016/j.jclinepi.2016.04.014
VanderWeele TJ (2019) Principles of confounder selection. Eur J Epidemiol 34:211–9. https://doi.org/10.1007/s10654-019-00494-6
Schisterman EF, Cole SR, Platt RW (2009) Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 20:488–95. https://doi.org/10.1097/EDE.0b013e3181a819a1
Hernán MA, Robins JM (2023) Causal Inference: What If. Chapman & Hall/CRC, Boca Raton
Kaaks R, Rinaldi S, Key TJ et al (2005) Postmenopausal serum androgens, oestrogens and breast cancer risk: the European prospective investigation into cancer and nutrition. Endocr Relat Cancer 12:1071–82. https://doi.org/10.1677/erc.1.01038
Tworoger SS, Zhang X, Eliassen AH et al (2014) Inclusion of endogenous hormone levels in risk prediction models of postmenopausal breast cancer. J Clin Oncol 32:3111–7. https://doi.org/10.1200/jco.2014.56.1068
Zhang X, Tworoger SS, Eliassen AH, Hankinson SE (2013) Postmenopausal plasma sex hormone levels and breast cancer risk over 20 years of follow-up. Breast Cancer Res Treat 137:883–92. https://doi.org/10.1007/s10549-012-2391-z
Zeleniuch-Jacquotte A, Bruning PF, Bonfrer JM et al (1997) Relation of serum levels of testosterone and dehydroepiandrosterone sulfate to risk of breast cancer in postmenopausal women. Am J Epidemiol 145:1030–8. https://doi.org/10.1093/oxfordjournals.aje.a009059
Zeleniuch-Jacquotte A, Shore RE, Koenig KL et al (2004) Postmenopausal levels of oestrogen, androgen, and SHBG and breast cancer: long-term results of a prospective study. Br J Cancer 90:153–9. https://doi.org/10.1038/sj.bjc.6601517
Sieri S, Krogh V, Bolelli G et al (2009) Sex hormone levels, breast cancer risk, and cancer receptor status in postmenopausal women: the ORDET cohort. Cancer Epidemiol Biomarkers Prev 18:169–76. https://doi.org/10.1158/1055-9965.Epi-08-0808
Berrino F, Muti P, Micheli A et al (1996) Serum sex hormone levels after menopause and subsequent breast cancer. J Natl Cancer Inst 88:291–6. https://doi.org/10.1093/jnci/88.5.291
Fourkala EO, Zaikin A, Burnell M et al (2012) Association of serum sex steroid receptor bioactivity and sex steroid hormones with breast cancer risk in postmenopausal women. Endocr Relat Cancer 19:137–47. https://doi.org/10.1530/erc-11-0310
Thomas HV, Key TJ, Allen DS et al (1997) A prospective study of endogenous serum hormone concentrations and breast cancer risk in post-menopausal women on the island of Guernsey. Br J Cancer 76:401–5. https://doi.org/10.1038/bjc.1997.398
Gunter MJ, Hoover DR, Yu H et al (2009) Insulin, insulin-like growth factor-I, and risk of breast cancer in postmenopausal women. J Natl Cancer Inst 101:48–60. https://doi.org/10.1093/jnci/djn415
Tin Tin S, Reeves GK, Key TJ (2021) Endogenous hormones and risk of invasive breast cancer in pre- and post-menopausal women: findings from the UK Biobank. Br J Cancer 125:126–34. https://doi.org/10.1038/s41416-021-01392-z
Trabert B, Sherman ME, Kannan N, Stanczyk FZ (2020) Progesterone and Breast Cancer. Endocr Rev 41:320–44. https://doi.org/10.1210/endrev/bnz001
Trabert B, Bauer DC, Buist DSM et al (2020) Association of circulating progesterone with breast cancer risk among postmenopausal women. JAMA Netw Open 3:e203645. https://doi.org/10.1001/jamanetworkopen.2020.3645
Acknowledgments
The authors thank Audrey Gicquiau for the measurement of the sex-steroid hormones and sex-hormone binding globulin, and Anne-Sophie Navionis for the measurement of the biomarkers of the insulin\insulin-like growth factor-signaling and inflammatory pathways. The authors also thank the participants of the Melbourne Collaborative Cohort Study. Cases and their vital status were ascertained through the Victorian Cancer Registry and the Australian Institute of Health and Welfare, including the National Death Index and the Australian Cancer Database
Disclaimer
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. Melbourne Collaborative Cohort Study (MCCS) cohort recruitment was funded by VicHealth and Cancer Council Victoria. The MCCS was further augmented by Australian National Health and Medical Research Council grants 209057, 396414 and 1074383 and by infrastructure provided by Cancer Council Victoria. Funding for IIG_2018_1730 was obtained from World Cancer Research Fund (WCRF UK), as part of the World Cancer Research Fund International grant programme. The reference standards for estradiol and testosterone were purchased and analyzed using funds from a NIH grant (NIH R01 CA207369) held by Dr Sue Hankinson at University of Massachusetts. Frances EM Albers and Makayla WC Low are each supported by a Research Training Program Scholarship from the Australian Government and the University of Melbourne. Makayla WC Lou is further supported by a scholarship from the Macau Special Administrative Region Government Higher Education Fund (Governo da Região Administrativa Especial de Macau Fundo do Ensino Superior).
Author information
Authors and Affiliations
Contributions
FEMA—Data curation, formal analysis, methodology, visualization, writing—original draft, writing—review & editing. MWCL—Data curation, methodology, writing—review & editing. SGD—Conceptualization, funding acquisition, methodology, supervision, writing—review & editing. CTVS—Methodology, supervision, writing—review & editing. SR—Conceptualization, data curation, funding acquisition, investigation, resources, writing—review & editing. VV—Methodology, writing—review & editing. AK—Conceptualization, funding acquisition, writing—review & editing. KAB—Conceptualization, funding acquisition, methodology, writing—review & editing. MJG—Conceptualization, funding acquisition, writing—review & editing. RLM—Conceptualization, funding acquisition, methodology, supervision, writing—review & editing. DRE—Conceptualization, data curation, funding acquisition, methodology, project administration, supervision, writing—review & editing. BML—Conceptualization, funding acquisition, methodology, supervision, writing—review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
The study protocol was approved by the Cancer Council Victoria Human Research Ethics Committee (Approval Number: CCV IEC 9001).
Consent to participate
All participants of the MCCS gave written informed consent.
Consent to publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Albers, F.E.M., Lou, M.W.C., Dashti, S.G. et al. Sex-steroid hormones and risk of postmenopausal estrogen receptor-positive breast cancer: a case–cohort analysis. Cancer Causes Control (2024). https://doi.org/10.1007/s10552-024-01856-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10552-024-01856-6