
Abstract
Background
Living in higher greenness level community has many benefits for pregnancy outcomes, however, few research have explored the relationship between greenness and spontaneous abortion (SAB). We aimed to analyze relationships between SAB and community greenness in Chinese pregnant women, and further assessed the modifying effects from air pollutants.
Methods
We studied 90 890 pregnant women from the China Birth Cohort Study from February 2018 to December 2021. We diagnosed SAB by certified obstetricians and gynecologists. The level of exposure to greenness during the first trimester was measured using the normalized difference vegetation index (NDVI) and the enhanced vegetation index (EVI). Particulate matter ≤ 2.5 μm (PM2.5), nitrogen dioxide (NO2) and ozone (O3) were used as proxies of ambient air pollution. Time-dependent multivariable adjusted Cox proportional hazards models, with gestational weeks as the time scale, were used to analyze the association between SAB and greenness. We additionally performed subgroup analyses stratified by age, urbanicity, research location, season of birth, temperature, humidity and air pollution levels.
Results
Lower SAB prevalence was related to living in greener places. A 0.1 unit increase in NDVI500m and EVI500m was significantly associated with a 12.3% (95% CI 9.9%, 15.5%) and 16.2% (95% CI 11.4%, 20.6%) lower risks of SAB, respectively. In sensitivity analysis, these relationships remained consistent. The associations were stronger among older, participants lived in the north of China and lived in places with higher PM2.5 and lower NO2 levels.
Conclusions
Our findings indicate significantly inverse associations between community greenness and SAB in Chinese pregnant women, especially for older and participants who live in the north of China, the PM2.5 and NO2 may modify the effects of greenness on SAB.
Similar content being viewed by others


Introduction
Spontaneous abortion (SAB) (or miscarriage), defined as the loss of an intrauterine pregnancy before viability, is one of the most serious adverse pregnancy outcomes [1]. Globally, there occur about 73 million SAB occur every year [2]. In China, the incidence rate of spontaneous abortion ranges from 3 to 5% [3,4,5]. SAB is related to both physical and psychological illnesses, including anxiety, depression, post-traumatic stress disorder, and suicide [6]. Also, having a history of SAB might raise the possibility of adverse pregnancy outcomes in subsequent pregnancies including preterm birth [1].
Nearly half of the world's population now resides in cities, and by 2050, it is anticipated that this number will exceed 70% (approximately 6.4 billion people) [7]. Rapid urbanization has reduced greenness levels, which is quite concerning for public health because exposure to higher levels of greenness might result in several positive health effects [8]. Plenty of studies have shown that greenness is related to several adverse birth outcomes [9,10,11], such as preterm birth, low birth weight, and small for gestational age [12,13,14], and no study has explored potential effects of greenness on SAB. Mechanistically, greenness may bring a series of health benefits, including decreased negative environmental exposures (e.g., air pollution and noise), promoted health-related activities (e.g., physical activity), improved psychophysiological recovery (e.g., reducing stress), and reduced adiposity [15]. These proposed mechanisms resemble those implicated in the pathophysiologic pathways of SAB. Therefore, it is biologically plausible that higher levels of greenness exposure are related to lower risk of SAB, and we test the hypothesis based on a birth cohort study conducted throughout China.
Materials and methods
Study participants
The study population was derived from the China Birth Cohort Study (CBCS). Briefly, CBCS is a prospective, longitudinal mega-cohort study performed between February 2018 and December 2021 among 35 research sites across 17 provinces and autonomous regions in China [16]. Pregnant women those with 6–13+6 weeks of gestation, planned to attend regular prenatal examination, delivered at the research location, and continued to reside in the same place for more than a year, were recruited. They were assigned with a questionnaire to collect data on demographic characteristics, health status, reproductive history, lifestyles, and environment factors at baseline. After enrollment, follow-up interviews were performed by certified doctors or nurses at gestational weeks at 20–23+6, 28–33+6 and delivery, respectively, to record information of pregnant outcomes. The study was approved by the Ethics Committee of Beijing Obstetrics and Gynecology Hospital, Capital Medical University (2018-KY-003–02). Written informed consent was obtained from all participants.
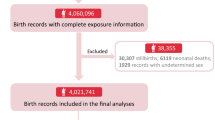
According to the current study, we included 106 087 potential study participants enrolled in CBCS. Of those, 90 890 (response rate = 85.7%) were included in the current analysis (Additional file 1: Figure S1), based on the following six criteria: (1) had resided locally for more than one year; (2) planned to attend routine antenatal examinations and deliver in the study site; (3) had no hepatitis B, syphilis, AIDS and other notifiable infectious diseases prescribed by the State; (4) were willing and able to sign informed consent; (5) had complete records of required information; (6) not voluntary abortion.
Outcome assessments
SAB was defined as a fetal loss occurring before completed gestation of 28 weeks [1]. In our study, certified obstetricians and gynecologists who strictly adhered to the above criterion made the diagnosis of SAB, which was then noted in medical records. Timing of concept is assessed by obstetricians based on the last menstrual period, while time to event is calculated based on the weeks of the outcome and the weeks of the last menstrual period, using the following formula: the weeks of the outcome—the weeks of the last menstrual period.
Exposure assessments
As measures of greenness, we utilized the normalized difference vegetation index (NDVI) and the enhanced vegetation index (EVI). The following formula was used for estimating NDVI as a ratio difference between measured canopy reflectance in the red (RED) and near infrared (NIR) bands, respectively: NDVI = (NIR–RED)/(NIR + RED). Similarly, EVI was determined using the formula: EVI = 2.5 × (NIR–RED)/(NIR + RED–7.5 × BLUE + 1), where BLUE stands for the reflectance of blue-region light. Higher values refer to more greenness for both indices, which have a range from -1 to 1. We used satellite images from Landsat8 OLI and TIRS at a 30 m × 30 m spatial resolution to calculate the NDVI and EVI around the centroid of each study participant through the latitude and longitude of the residential address. The USGS EarthExplorer (https://earthexplorer.usgs.gov/) provided remote sensing data for the year 2016 [17]. We assessed the NDVI and EVI every 16 days and then averaged them during the first trimester (0–13+6 weeks). For the initial analysis, we used the NDVI and EVI values with the 500 m buffer. Other metrics and buffers were presented in sensitivity analyses as well.
The China High Air Pollutants (CHAP) dataset was used to get full-coverage ground-level PM2.5, NO2, and O3 concentrations with 0.1° × 0.1° spatial resolution. Details of the air pollutants exposure assessments have been described elsewhere [18,19,20]. In short, to estimate the ambient PM2.5, NO2, and O3 concentrations, an extensive collection of data from ground-based measurements, satellite remote sensing products, model simulations, and atmospheric reanalysis was fitted using artificial intelligence algorithms. The assessments were then validated using the tenfold cross-validation approach by measuring the adjusted coefficient of determination (R2) and root mean squared error (RMSE). Air pollutants concentrations were assigned to each participant according to their residential addresses, and the measurement period of air pollutants concentrations is in the first trimester.
We collected daily average temperature and humidity from the China Meteorological Data Service Center (CMDC, http://data.cma.cn/en). Then, we calculated the average ambient temperature and humidity of first trimester for every participants.
Potential confounders and mediators
We used self-filled questionnaires to collect the following information: (a) characteristics of pregnant women, including age (years), ethnicity (Han vs. others), education (high school or lower versus college vs. master or higher), annual family income (< 100 000 CNY vs. 100 000–200 000 CNY vs. > 200 000 CNY), residential region (South vs. North) and residential address; (b) habits of life, such as alcohol intake (yes vs. no) and maternal smoke exposure (yes vs. no); and (c) present clinical information, including parity (0 vs. ≥ 1), pre-pregnancy BMI (kg/m2) and season of pregnancy outcome (spring vs. summer vs. fall vs. winter).
Pre-pregnancy BMI was calculated as follows: weight in kilos divided by square of height in meters. The height and weight for three month before pregnancy were reported by pregnant women. The Chinese Statistical Yearbooks (http://www.stats.gov.cn) were used to identify urbanicity (urban vs. rural). The 35 member centers were distinguished as north and south based on the Qinling Mountain-Huaihe River Line (near latitude 33°N), a natural boundary for regional demarcation between North and South China [21].
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) and categorical variables as frequency with percentage, respectively. We used the Chi-square test or t-test to test the differences of characteristics between SAB and non-SAB. Time-dependent multivariable adjusted Cox proportional hazards models, with gestational weeks as the time scale, were constructed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of explore the associations between residential greenness (NDVI500m and EVI500m) and SAB after adjusting for potential confounding variables, including age, pre-pregnancy BMI, education, annual family income, ethnicity, parity, season of birth, region and PM2.5. From the Cox model fit we have: Y(t) = β1∙age(t) + β2∙pre-pregnancy BMI + β3∙education(t) + β4∙annual family income(t) + β5∙ethnicity + β6∙parity + β7∙season of birth(t) + β8∙region + β9∙PM2.5 + β10∙NDVI500m, β is a vector of regression coefficients [22].
We used the restricted cubic spline (RCS) function to test the potential nonlinear associations between greenness exposure during the first trimester and risk of SAB, with three knots set at the 10th, 50th and 90th percentiles.
Subgroups analyses were also performed according to maternal age, pre-pregnancy BMI, annual family income, air pollutants levels, temperature and humidity to identify whether they were potential modifiers of associations between greenness and SAB. Maternal age was categorized as high risk group (≥ 35 years) and low risk group (< 35 years). Pre-pregnancy BMI was categorized as normal group (< 24 kg/m2) and overweight/obesity group (≥ 24 kg/m2) [23], and annual family income as low income group (< 100 000 Yuan), middle income group (100 000–200 000 Yuan) and high income group (> 200 000 Yuan). A lower exposure group and a higher exposure group were designed for PM2.5, NO2, and O3. Lower exposure represented less than the first interquartile range of air pollution, while higher exposure represented more than the first interquartile range of air pollution; the first interquartile range in PM1: 23.535 µg/m3; in PM2.5: 29.732 µg/m3; in PM10: 43.458 µg/m3; in NO2: 25.548 µg/m3; and in O3: 62.089 µg/m3. Temperature and humidity were categorized as lower group and higher group by median (18.1 °C and 65.3%, respectively). We repeated the analysis for each subgroup and P-values for interactions were reported.
Sensitivity analyses
We performed two sensitivity analyses to assess the robustness of our findings. First of all, we used the other two buffers (namely 250 m and 1 000 m buffers for NDVI) in the model. Then, we investigated the relationship between residential greenness and SAB after excluding multipara and participants who smoke or drink alcohol.
All analyses were conducted using R (version 4.0.3, R Foundation for Statistical Computing). A two-tailed P-value < 0.05 was considered as statistically significant.
Results
Population description
Table 1 shows the descriptive statistical characteristics of the entire cohort (n = 90 890), with a total of 2 817 (3.1%) were detected as SAB. Compared with the non-SAB participants, the patients with SAB were older and had a higher proportion of education level and annual family income.
Greenness and air pollutants exposure
In terms of environmental factors, pregnant women with SAB lived in areas with lower greenness levels and higher air pollution levels during the first trimester, except for PM2.5. Pregnant women with SAB live in environments with lower PM2.5 levels. The mean NDVI500m and EVI500m in non-SAB participants was 0.296 and 0.181, respectively, and in the SAB cases was 0.283 and 0.172, respectively. PM2.5, NO2 and O3 in non-SAB participants was 42.333 μg/m3, 33.827 μg/m3 and 91.186 μg/m3, respectively, and in the SAB cases was 42.054 μg/m3, 34.780 μg/m3 and 92.324 μg/m3, respectively. The median of PM2.5, NO2 and O3 was 37.778 μg/m3, 32.556 μg/m3 and 85.444 μg/m3, respectively (Additional file 1: Table S1).
Greenness and spontaneous abortion
As shown in Additional file 1: Figure S2, NDVI500m had no significant nonlinear associations with SAB (P > 0.05). Our research showed a straight line.
The associations between residential greenness and SAB are shown in Table 2. In the unadjusted model, for 0.1 unit increase in NDVI500m, the HR for SAB was 0.916 (0.889, 0.944). After fully multivariate adjustment, for every 0.1 unit increase in the NDVI500m, the risk of SAB (HR = 0.877, 95% CI 0.845–0.911 in model1; HR = 0.925, 95% CI 0.852–0.959 in model2; HR = 0.912, 95% CI 0.877–0.948 in model3) significantly decreased. In model 1, compared with Q1, the protection effect of the greenness measured by NDVI500m was strongest in Q4 (HR = 0.686, 95% CI 0.604–0.778). In model 2 and model 3, the protection effect of the greenness measured by NDVI500m was strongest in Q3 (HR = 0.815, 95% CI 0.725–0.916 and HR = 0.766, 95% CI 0.673–0.871, respectively). Among all three models, there is no statistical significance in Q2, and the protection effect is very closed in Q3 and Q4. The same trend can also be observed in EVI500m.
The Kaplan–Meier survival curves for NDVI500m and EVI500m with different interquartile range groups are shown in Additional file 1: Fig. S3–S4.
Sensitivity analyses
NDVI250m and NDVI1000m were used in sensitivity analysis, which indicated that the correlations were mainly consistent (Additional file 1: Table S2). Additionally, estimates remained consistent after excluding individuals who smoked, drank alcohol, or had multipara (Additional file 1: Tables S3–S5).
Effect modification
Figure 1 shows associations for greenness exposures and SAB according to potential effect modifiers. The associations between greenness and subsequent SAB risk were more pronounced among participants with older age than those younger than 35 years at the baseline. In addition, the relationship between residential greenness and SAB was stronger among participants lived in north of China and those whose birth outcomes occur in spring and winter. We also found that the relationship between residential greenness and SAB was stronger in participants with higher PM2.5 and lower NO2. The results of stratified analysis by urbanicity, temperature, humidity and O3 were not statistically significant.

Associations between per 0.1 unit increase in NDVI500m and SAB by age, urbanicity, research location, season of birth, temperature, humidity and air pollutant level (n = 90 890)*. *The model was adjusted for maternal age, education, pre-pregnancy BMI, ethnicity, annual family income, parity, season of birth, region, particle with aerodynamic diameter less than 2.5 μm (PM2.5), nitrogen dioxide (NO2) and ozone (O3).
Discussion
Key findings
In our large population-based cohort study, we found that increased greenness exposure during the first trimester was significantly associated with lower risk of SAB, especially in older and participants lived in the north of China, and this association showed a linear dose–response relationship. In addition, concentrations of PM2.5 and NO2 may modify the effects of greenness on SAB.
Comparison with prior studies and interpretations
To our knowledge, this is the first epidemiological study that demonstrates a relationship between early prenatal exposure to community greenness and SAB. Only one study performed by Sun et al. [24] found greenness can attenuate the effect of temperature on SAB, which supported our findings of protective effects of gestational greenness exposure on SAB. Besides SAB, many studies have estimated the effects of greenness exposure on other adverse pregnancy outcomes, including small for gestational age (SGA), low birth weight (LBW) and preterm birth (PTB) [13, 25,26,27,28], and most of indicated a beneficial effects of greenness on these outcomes. The prior studies combined with ours indicated that living greener areas may be beneficial for birth outcomes, especially our large and well-represented study firstly find a protective association for SAB.
Underlying mechanism
Notwithstanding that the biological mechanisms of the relationship between SAB and residential greenness are still unclear, several biopsychosocial pathways have been proposed. First of all, those who live near green space are more likely to exercise, which can lower the risk of obesity, which has been correlated to an increased risk for SAB [29, 30]. Stratification analyses in our study confirmed this hypothesis by finding the higher the pre-pregnancy BMI, the less protective effect green space has on SAB. Second, green space may decrease the negative effects of air pollution on the environment, such as PM2.5, which has been widely discussed as risk factors for SAB [31,32,33]. According to our findings, PM2.5 can attenuate the negative relationship between increasing gestational greenness exposure and a reduced risk of SAB, which is in line with the proposed hypothesis. Third, according to studies, living in greener places may also help with reduced mental stress and concentration problems, improved social interaction, increased microbial diversity, and altered human microbiota composition [8, 15]. We were unable to explore these mechanisms as potential moderators of the relationship between greenness and SAB, however, given that our study's data were lacking. More mechanistic research is, therefore, required to confirm the underlying mechanisms.
Susceptible populations
We found that the association between greenness exposure during the first trimester and the risk of SAB was stronger in the north of China. To our knowledge, no studies have been done to examine the relationship between SAB and being exposed to greenness while pregnant. Nonetheless, our results were not surprising. Compared with southern China, northern China urbanizes more rapidly [34]. For example, areas with high urbanization have better access to healthcare and community involvement, which attenuate the prevalence of SAB [35]. The relationship may also be explained by socioeconomic status factors [36, 37], such as income and education. People with higher income level and higher education level are more likely to participate in physical exercise and maintain a healthy lifestyle, thus attenuating the risk of SAB. In addition, due to the more suitable temperature and humidity for vegetation growth, the greenness level in southern China is better than that in the north. Therefore, there is a slight change in the greenness level in the north, the result will be more significant changes. We also detected that older seems more vulnerable than younger in the association between greenness and SAB. Furthermore, the relationship between residential greenness and SAB was stronger among participants whose birth outcomes occur in spring and winter. Since the overall greenness level in spring and winter is lower than that in summer and fall, the change of greenness level in spring and winter will make the results more significant.
In addition, we noted the modifying effect of air pollution on the relationship between exposure to gestational greenness and the risk of SAB, which the effect of greenness exposure were stronger in higher levels of PM2.5, and lower levels of NO2. Although we were unable to search for any studies examining the impact of air pollution on residential greenness and SAB, the similar reason have been explained in studies of greenness and other adverse birth outcomes [13, 38]. The possible reason is that the risk of SAB is increased by air pollution [1], so higher levels of air pollutants may lead to higher prevalence of SAB. Given that limited evidence is available, additional research is required to confirm our findings.
Strengths and limitations
Our study has several strengths. First, this prospective cohort study eventually included a total of 90,890 participants, it includes 17 Chinese provinces and autonomous areas, to our best knowledge, this is the largest cohort study of greenness during pregnancy and SAB, which reduce potential selection bias. Additionally, clinically verified diagnoses were utilized to mitigate outcome misclassification, and health professionals delivered a face-to-face study questionnaire to minimize exposure and covariate misclassification. Second, we calculated NDVI and EVI by the latitude and longitude of personal address, and the average exposure during the first trimester was calculated accurately which has been proved to be more accurate compared with studies that used residential postal code [39]. Third, we conducted detailed sensitivity studies to assess the reliability of the results.
Our study also had several limitations to acknowledge. First, this study did not collect information on the work addresses of the participants, which could have led to a potential misclassification bias between participants who remained employed during pregnancy and those who did not. Second, we didn't have enough information about individual anxiety, stress and depression to test the mechanisms in previous studies. Third, we measured greenness levels using the vegetation indices NDVI and EVI, which do not provide information on the kinds of vegetation or the accessibility of green space. Fourth, even though we considered and adjusted for a variety of covariates, there remains the possibility of unmeasured confounding, such as area-level GDP and population density, which may lead to potential selection bias. Fifth, since the miscarriage rate is higher in earlier pregnancies, the wide range of gestation age at enrollment may poses a risk of selection bias. Sixth, as we are unable to recruit miscarriage cases from 6 gestational weeks ago, so the incidence rate will be slightly lower, and it will inevitably lead to selection bias.
Conclusions
In conclusion, lower SAB prevalence was related to higher levels of community greenness, especially among older and pregnant women who live in the north of China, the PM2.5 and NO2 may modify the effects of greenness on SAB. As global urbanization intensification, our findings have critical public health implications. However, to protect pregnant women from adverse birth outcomes, particularly in the north of China with rapid urbanization, it is important to further examine the positive benefits of greenness on SAB through well-designed longitudinal research.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due the authors do not have access to the database.
Abbreviations
- SAB:
-
Spontaneous abortion
- NDVI:
-
The normalized difference vegetation index
- EVI:
-
The enhanced vegetation index
- PM1 :
-
Particulate matter ≤ 2.5 μm
- PM2.5 :
-
Particulate matter ≤ 2.5 μm
- PM10 :
-
Particulate matter ≤ 2.5 μm
- NO2 :
-
Nitrogen dioxide
- O3 :
-
Ozone
- CBCS:
-
The China Birth Cohort Study
- NIR:
-
Near infrared
- CHAP:
-
China High Air Pollutants
- RMSE:
-
Root mean squared error
- SD:
-
Standard deviation
- BMI:
-
Body mass index
- CNY:
-
China Yuan
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- RSC:
-
The restricted cubic spline
- SGA:
-
Small for gestational age
- LBW:
-
Low birth weight
- PTB:
-
Preterm birth
References
Quenby S, Gallos ID, Dhillon-Smith RK, Podesek M, Stephenson MD, Fisher J et al (2021) Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet 397(10285):1658–1667
World Health Organization. 2013. Urban Population Growth. http://www.who.int/gho/urban_health/situation_trends/urban_population_growth_text/en/. Accessed 20 Jun 2023.
Hu X, Miao M, Bai Y, Cheng N, Ren X (2018) Reproductive factors and risk of spontaneous abortion in the Jinchang Cohort. Int J Environ Res Public Health 15(11):2444
Xu Q, Yang Y, Liu F, Wang L, Wang Q, Shen H et al (2020) Preconception Hb concentration with risk of spontaneous abortion: a population-based cohort study in over 3·9 million women across rural China. Public Health Nutr 23(16):2963–2972
Hu CY, Yang XJ, Hua XG, Jiang W, Huang K, Chen HB et al (2021) Risk factors for spontaneous abortion from a prevention perspective in rural China: a population-based follow-up study. J Matern Fetal Neonatal Med 34(16):2583–2591
Sugiura-Ogasawara M, Ebara T, Yamada Y, Shoji N, Matsuki T, Kano H et al (2019) Adverse pregnancy and perinatal outcome in patients with recurrent pregnancy loss: Multiple imputation analyses with propensity score adjustment applied to a large-scale birth cohort of the Japan Environment and Children’s Study. Am J Reprod Immunol 81(1):e13072
World Health Organization. 2021. Abortion. https://www.who.int/news/item/11-12-2010-urban-planning-essential-for-public-health. Accessed 20 Jun 2023.
Yang BY, Zhao T, Hu LX, Browning M, Heinrich J, Dharmage SC et al (2021) Greenspace and human health: an umbrella review. Innovation (Camb) 2(4):100164
Lee PC, Wu CD, Tsai HJ, Tsai HY, Lin SH, Wu CK et al (2021) Residential greenness and birth outcomes: evaluating the mediation and interaction effects of particulate air pollution. Ecotoxicol Environ Saf 211:111915
Cusack L, Larkin A, Carozza S, Hystad P (2017) Associations between residential greenness and birth outcomes across Texas. Environ Res 152:88–95
Margerison CE, Pearson AL, Lin Z, Sanciangco J (2021) Changes in residential greenness between pregnancies and birth outcomes: longitudinal evidence from Michigan births 1990–2012. Int J Epidemiol 50(1):190–198
Zhang L, Shi S, Wu S, Yang Y, Xu J, Zhang Y et al (2022) Effects of greenness on preterm birth: a national longitudinal study of 3.7 million singleton births. Innovation 3(3):100241
Laurent O, Benmarhnia T, Milesi C, Hu J, Kleeman MJ, Cockburn M et al (2019) Relationships between greenness and low birth weight: investigating the interaction and mediation effects of air pollution. Environ Res 175:124–132
Fong KC, Kloog I, Coull BA, Koutrakis P, Laden F, Schwartz JD et al (2018) Residential greenness and birthweight in the state of Massachusetts, USA. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph15061248
Markevych I, Schoierer J, Hartig T, Chudnovsky A, Hystad P, Dzhambov AM et al (2017) Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ Res 158:301–317
Yue W, Zhang E, Liu R, Zhang Y, Wang C, Gao S et al (2022) The China birth cohort study (CBCS). Eur J Epidemiol 37(3):295–304
Luo YN, Yang BY, Zou Z, Markevych I, Browning M, Heinrich J et al (2022) Associations of greenness surrounding schools with blood pressure and hypertension: a nationwide cross-sectional study of 61,229 children and adolescents in China. Environ Res 204(Pt A):112004
Wei J (2020) Improved 1 km resolution PM; estimates across China using enhanced space-time extremely randomized trees. Atmospheric Chem Phys 20(6):3273–89
Wei J, Li Z, Li K, Dickerson R, Cribb M (2021). Full-coverage mapping and spatiotemporal variations of near-surface ozone pollution from 2013 to 2020 across China. Remote Sensing of Environ 270:112775
Wei J, Li Z, Lyapustin A, Sun L, Peng Y, Xue W, Tianning S, Cribb M (2021) Reconstructing 1-km-resolution high-quality PM2.5 data records from, 2000 to 2018 in China: spatiotemporal variations and policy implications. Remote Sensing of Environ Interdisciplinary J. https://doi.org/10.1016/j.rse.2020.112136
Wu Z, Jiang Z, Li T, Xie C, Zhao L, Yang J et al (2021) Structural variants in the Chinese population and their impact on phenotypes, diseases and population adaptation. Nat Commun 12(1):6501
Xu R, Luo Y, Glynn R, Johnson D, Jones KL, Chambers C (2014) Time-dependent propensity score for assessing the effect of vaccine exposure on pregnancy outcomes through pregnancy exposure cohort studies. Int J Environ Res Public Health 11(3):3074–3085
Jung CC, Su HJ, Liang HH (2016) Association between indoor air pollutant exposure and blood pressure and heart rate in subjects according to body mass index. Sci Total Environ 539:271–276
Sun X, Luo X, Cao G, Zhao C, Xiao J, Liu X et al (2020) Associations of ambient temperature exposure during pregnancy with the risk of miscarriage and the modification effects of greenness in Guangdong. China Sci Total Environ 702:134988
Ebisu K, Holford TR, Bell ML (2016) Association between greenness, urbanicity, and birth weight. Sci Total Environ 542(Pt A):750–756
Glazer KB, Eliot MN, Danilack VA, Carlson L, Phipps MG, Dadvand P et al (2018) Residential green space and birth outcomes in a coastal setting. Environ Res 163:97–107
Agay-Shay K, Peled A, Crespo AV, Peretz C, Amitai Y, Linn S et al (2014) Green spaces and adverse pregnancy outcomes. Occup Environ Med 71(8):562–569
Dzhambov AM, Markevych I, Lercher P (2018) Greenspace seems protective of both high and low blood pressure among residents of an Alpine valley. Environ Int 121(Pt 1):443–452
Huang WZ, Yang BY, Yu HY, Bloom MS, Markevych I, Heinrich J et al (2020) Association between community greenness and obesity in urban-dwelling Chinese adults. Sci Total Environ 702:135040
Luo YN, Huang WZ, Liu XX, Markevych I, Bloom MS, Zhao T et al (2020) Greenspace with overweight and obesity: A systematic review and meta-analysis of epidemiological studies up to 2020. Obes Rev 21(11):e13078
Rojas-Rueda D, Morales-Zamora E, Alsufyani WA, Herbst CH, AlBalawi SM, Alsukait R et al (2021) Environmental risk factors and health: an umbrella review of meta-analyses. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph18020704
Cheng Y, Wang P, Zhang L, Shi H, Li J, Meng X et al (2023) Ozone exposure during pregnancy and risk of gestational hypertension or preeclampsia in China. JAMA Netw Open 6(4):e236347
Dzhambov AM, Tilov B, Makakova-Tilova D, Dimitrova DD (2019) Pathways and contingencies linking road traffic noise to annoyance, noise sensitivity, and mental Ill-Health. Noise Health 21(103):248–257
Sun Y, Zhang M, Chen S, Zhang W, Zhang Y, Su S et al (2023) Potential impact of ambient temperature on maternal blood pressure and hypertensive disorders of pregnancy: A nationwide multicenter study based on the China birth cohort. Environ Res 227:115733
Xiao X, Gao M, Zhou Y, Xu SL, Knibbs LD, Heinrich J et al (2022) Is greener better? Associations between greenness and birth outcomes in both urban and non-urban settings. Int J Epidemiol 51(1):88–98
Casey JA, James P, Rudolph KE, Wu CD, Schwartz BS (2016) Greenness and birth outcomes in a range of Pennsylvania communities. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph13030311
Eriksson C, Lind T, Ekstrom S, Gruzieva O, Georgelis A, Bergstrom A et al (2019) Neighbourhood greenness and birth outcomes in a Swedish birth cohort—a short communication. Health Place 57:200–203
Lin L, Li Q, Yang J, Han N, Chen G, Jin C et al (2020) The associations of residential greenness with fetal growth in utero and birth weight: a birth cohort study in Beijing. China Environ Int 141:105793
Hystad P, Davies HW, Frank L, Van Loon J, Gehring U, Tamburic L et al (2014) Residential greenness and birth outcomes: evaluating the influence of spatially correlated built-environment factors. Environ Health Perspect 122(10):1095–1102
Acknowledgements
We appreciate the cooperation of all participating subjects in this study who have been very generous with their time and assistance. Finally, we acknowledge the efforts of all who did the fieldwork.
Funding
This work was supported by the National Key Research and Development Program of China (2016YFC1000101), the National Natural Science Foundation of China (no. 81972992), the Guangzhou Science and Technology Project (no. 202201011545) and R&D Program of Beijing Municipal Education Commission (KM202310025006).
Author information
Authors and Affiliations
Contributions
YC: provided conception and design of research; acquisition, analysis, and interpretation of data; drafted the manuscript. SG: provided conception and design of research; acquisition, analysis, and interpretation of data; revised the manuscript. BY: provided conception and design of research; acquisition, analysis, and interpretation of data; revised the manuscript. WY: acquisition and analysis. SS: acquisition and interpretation of data. EZ: acquisition and analysis. JL: acquisition and interpretation of data. SX: acquisition and interpretation of data. YZ: revised the manuscript. ZZ: revised the manuscript. RL: provided conception and design of research; revised the manuscript. GD: provided conception and design of research; revised the manuscript. CY: provided conception and design of research; analysis, and interpretation of data.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Beijing Obstetrics and Gynecology Hospital, Capital Medical University (2018-KY-003–02). Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Distributions of environmental factors during first trimester (n=90 890). Table S2. Associations between NDVI in different buffers and SAB (n = 90 890). Table S3. Associations between greenness and SAB in sensitivity analyses. Table S4. Associations between greenness and SAB in sensitivity analyses. Table S5. Associations between greenness and SAB in sensitivity analyses. Figure S1. Flow chart of participant recruitment. Figure S2. Nonlinear associations between greenness and spontaneous abortion (SAB). Figure S3. Kaplan-Meier survival curves of NDVI500m(log-rank test: P<0.001). Figure S4. Kaplan-Meier survival curves of EVI500m (log-rank test: P<0.001).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cui, Y., Gao, S., Yang, B. et al. Associations of residential greenness exposure during early pregnancy with the risk of spontaneous abortion: the China Birth Cohort Study. Environ Sci Eur 36, 33 (2024). https://doi.org/10.1186/s12302-024-00869-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12302-024-00869-x