
Abstract
Objective
To evaluate factors associated with borderline/clinical range Child Behavior Checklist (CBCL) scores in opioid-exposed children.
Study design
Retrospective study of 94 children with prenatal opioid exposure evaluated with the CBCL at age 2 years.
Results
Twenty-eight children (30%) had borderline/clinical findings on the CBCL, with 27% scoring borderline/clinical for Externalizing Problems. In the multivariable model, lower Bayley-III motor scores and discharge home with mother with safety plan were associated with borderline/clinical Externalizing Problems. Medication treatment for neonatal opioid withdrawal syndrome (NOWS) was associated with normal Externalizing Problems scores. Treatment with clonidine or phenobarbital was associated with scores in the normal range in all broadband CBCL measures.
Conclusion
Specific factors are associated with behavioral and emotional challenges measured by borderline/clinical CBCL scores among opioid-exposed children.
Similar content being viewed by others
Introduction
Neonatal opioid withdrawal syndrome (NOWS) rates have increased over the last decade in parallel with a worsening national opioid crisis. Children with history of prenatal opioid exposure have been shown to experience higher rates of cognitive, language, behavioral, attention, emotional regulation, and developmental problems than unexposed children [1]. Development of these emotional and behavioral disorders is likely multifactorial. Previous studies have shown an association between socioeconomic status and behavioral and emotional problems in opioid-exposed children as identified by the CBCL, but these studies report on school-aged and adolescent populations outside of the United States, and results may not be generalizable [2, 3]. Studies within the United States have typically considered socioeconomic risk factors as confounding variables rather than as predictors or modifiers of neurodevelopmental outcomes among opioid-exposed children [4]. Our previous retrospective cohort study identified custody status (with mother versus foster/adoptive families) as a risk factor for lower scores on the Bayley cognitive subscale [5]. However, little is known about how contextual factors, including biological risk, maternal and caregiver environment, and severity of withdrawal, impact risk for developing behavioral problems in opioid-exposed children.
Here, we determine the prevalence of behavioral and emotional problems in a retrospective cohort of opioid-exposed children and analyze the associations between development of these problems and specific clinical or social risk factors. In this exploratory, hypothesis-generating pilot study, we hypothesized that higher withdrawal severity and custody status would be associated with behavioral or emotional problems at age 2 years in opioid-exposed children.
Materials/Subjects and methods
In this study, we administered the Child Behavior Checklist (CBCL) to caregivers of children seen in our institution’s NOWS Follow-Up Clinic between 2016 and 2021 around the 2-year clinic visit. The CBCL is a caregiver-administered questionnaire from the Achenbach System of Empirically Based Assessment (ASEBA) that can be completed for children as young as 1 ½ years and is comprised of 99 items that broadly screen for behavioral and emotional problems [6]. It includes 7 syndrome scales that are grouped into Internalizing Problems (emotionally reactive, anxious/depressed, withdrawn, somatic complaints) and Externalizing Problems (attention problems, aggressive behavior). Scores are scaled to normative standards and represented by T scores, which are then categorized into normal, borderline, or clinical range scores, per the ASEBA manual. Borderline scores refer to being at risk for a behavioral problem, while scores in the clinical range indicate a likely need for services.
All infants born in Cincinnati area hospitals with prenatal opioid exposure, determined by maternal history, universal maternal urine toxicology screen at delivery, and/or infant toxicology screen after birth, were eligible to be seen in our follow-up clinic. Children were followed to age 2 or 3 years with standardized developmental, vision, nutritional, and behavioral assessments. A total of 94 children completed follow-up and behavioral assessments between 2016 and 2021. Power analysis was not performed prior to the study due to lack of trustworthy effect size parameters. In addition, our single institution data collection limited the number of eligible subjects available. Therefore, we used this convenient sample of all patients in the specified time period for this pilot study. Data regarding infant characteristics, maternal characteristics, socioeconomic factors, substance exposure and withdrawal symptoms were extracted from the electronic medical records. Infant characteristics included gestational age at birth, chronological age at time of CBCL completion, sex, birth weight, head circumference, infant race/ethnicity, and Bayley-III scores (measured around 2 years corrected age). Maternal characteristics included maternal age, maternal smoking during pregnancy, and hepatitis C infection. Our data collection did not specify if smoking data described as packs per day pertained to average packs per day smoked during pregnancy or packs per day smoked at the time of screening. Socioeconomic factors included maternal or primary caregiver education, type of health insurance, relationship status of parents, and custody plan at hospital discharge. Custody plans include discharged with mother, discharged with mother and a safety plan, and discharged to foster care. A “safety plan” was defined in accordance with the Ohio Department of Job and Family Services Manual, whereby specific interventions within the home are agreed upon to control threats of serious harm without changing the legal custody status of the child [7]. Substance exposures included methadone, buprenorphine, short-acting opioids (such as morphine, heroin, fentanyl, or other prescription opioid pain medications), marijuana, cocaine, amphetamines, selective serotonin reuptake inhibitors (SSRIs), and other. Data regarding whether the infant required pharmacologic treatment for withdrawal, level of treatment for NOWS (no treatment versus opioid only vs opioid plus adjunctive medication), duration of opioid treatment, and length of birth hospital stay were also analyzed.
Statistical analysis
The primary outcome was a borderline/clinical range score (versus normal score) for the broadband measures Internalizing Problems, Externalizing Problems, or Total Problems. For the purpose of this exploratory study with a small sample size, we grouped borderline and clinical range scores together to help identify children who would need closer follow-up, being at risk for these problems or benefitting from referral for additional services. Descriptive statistics were reported for clinical and social descriptors using median with interquartiles (25th and 75th percentiles) for continuous variables and frequency with percentages for categorical variables. Bivariate analysis of these variables with the primary outcome was performed using Wilcoxon rank sum test for continuous variables to accommodate limited sample size and potential deviations from the normal distribution. Fisher’s exact test wase done for categorical variables due to small sample size.
A logistic regression model was used to assess the potential association between each risk factor and borderline/clinical scores for each of the following broadband measures: Internalizing Problems, Externalizing Problems, and Total Problems. A logistic regression model was also used to evaluate the association between risk factors and a borderline/clinical range outcome on any one of the three broadband measures. Odds ratio, confidence intervals and p-values were reported. Multivariable models were then built through stepwise variable selection procedures using all infant characteristics, maternal characteristics, socioeconomic factors and substance exposure variables. The final model contained significant terms with 0.1 significance entry and stay level. Adjusted odds ratio (aOR), confidence intervals and p-values were reported. A 2-sided p-value < 0.05 was used to determine the significance of variables in all analyses. Observations with missing data in any of the variables involved in a model were excluded from the analysis. Given the exploratory nature of this study, we did not adjust for multiple comparisons. Data analyses were performed using SAS version 9.4 (SAS Institute, Cary, North Carolina). The SAS codes for analysis are available upon request.
Ethics approval
This study was reviewed by the Cincinnati Children’s Hospital Medical Center Institutional Review Board and determined to be exempt as it posed minimal risk; thus, it was allowed to be conducted using waiver of informed consent.
Results
Our cohort included 94 children, of whom 40 (43%) were male and 84 (89%) received pharmacologic treatment for NOWS. Demographic information for the cohort is shown in Table 1. The median gestational age at birth was 38.1 (interquartiles: 36.3, 39.4) weeks with range 31 to 42 weeks. The median chronological age and median adjusted age at completion of the CBCL were 24.6 (23.4, 25.8) months and 23.9 (22.8, 25.2) months, respectively. Children were most commonly exposed prenatally to short-acting opioids (such as morphine, heroin, and fentanyl) (77%), followed by methadone or buprenorphine (60%). Twenty-eight children (30%) had at least one borderline/clinical score on the CBCL. Twelve children (13%) had borderline/clinical scores for Internalizing Problems, 25 (27%) for Externalizing Problems, and 10 (11%) for Total Problems.
Univariate analysis
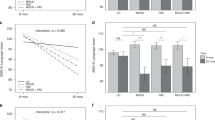
In the univariate analysis for associations between binary CBCL outcomes and Bayley-III subscales, higher Bayley-III motor scores were associated with decreased odds of having at least one borderline/clinical CBCL outcome (OR = 0.948, 95% CI = 0.904–0.994, p = 0.029; Table 2). Higher Bayley-III motor and cognitive scores were associated with a decreased odds of a borderline/clinical score for Internalizing Problems (OR = 0.932, 95% CI = 0.873–0.994, p = 0.033; OR = 0.921, 95% CI = 0.855–0.992, p = 0.030, respectively; Table 2). Higher Bayley-III motor scores were associated with a decreased odds of a borderline/clinical score for Externalizing Problems (OR = 0.947, 95% CI = 0.902–0.995, p = 0.031; Table 2). Higher Bayley-III total language and cognitive scores were associated with a decreased odds of a borderline/clinical score for Total Problems (OR = 0.937, 95% CI = 0.889–0.986, p = 0.012; OR = 0.925, 95% CI = 0.859–0.997, p = 0.041; Table 2). Bayley-III motor scores showed a similar association with borderline/clinical Total Problems score, although did not reach statistical significance (OR = 0.945, 95% CI = 0.886–1.008, p = 0.086; Table 2).
Among the social risk factors assessed, only discharge home with mother with safety plan was associated with having any borderline/clinical range outcome (OR = 5.727, 95% CI = 1.319–24.870, p = 0.020; Table 2) and with a borderline/clinical score for Externalizing Problems (OR = 6.947, 95% CI = 1.586–30.419, p = 0.010; Table 2).
Multivariable model
In the selected multivariable models, children born to mothers who smoked more cigarettes per day had an increased odds of having at least one borderline/clinical CBCL score (aOR = 11.1, 95% CI = 1.3–97.1, p = 0.030; Table 3). Treatment of NOWS with clonidine or phenobarbital as adjunctive therapy in addition to opioid therapy was associated with a decreased odds of having a borderline/clinical CBCL score (aOR = 0.045, 95% CI = 0.004–0.466, p = 0.009; Table 3). Higher Bayley-III motor scores were associated with a decreased odds of a borderline/clinical range score for Externalizing Problems (aOR = 0.93, 95% CI = 0.89–0.99, p = 0.020; Table 3). In other words, a borderline/clinical range score for Externalizing Problems was associated with lower Bayley-III motor scores, as well as with being discharged with mother and safety plan (aOR = 12.05, 95 CI = 2.37–61.24, p = 0.003; Table 3). Pharmacologic treatment for NOWS was associated with a decreased odds of Externalizing Problems (aOR = 0.16, 95% CI = 0.04–0.76, p = 0.021; Table 3).
Discussion
Here we described the use of the CBCL, a caregiver-administered questionnaire that identifies behavioral and emotional dysregulation based on the presence of problem behaviors, in a cohort of children with prenatal opioid exposure around 2 years of age. We identified a high prevalence of behavioral and emotional challenges, with 30% of our cohort having at least one borderline or clinical range score on the CBCL. The majority of studies thus far on long-term outcomes in opioid-exposed children have shown that when problems are present, they tend to occur across multiple domains [8,9,10,11] Similarly, we repeatedly found that among our cohort, higher scores on multiple subscales of the Bayley-III assessment were associated with a decreased odds of a borderline/clinical score for different CBCL outcomes (i.e. lower scores on multiple Bayley-III subscale assessments were associated with borderline/clinical scores for different CBCL outcomes). While our study does not draw causal conclusions, our findings add to growing literature suggesting that prenatal opioid exposure portends risk for long-term effects on motor, language, cognitive, emotional and behavioral development.
Severity of withdrawal symptoms did not impact development of behavioral and emotional problems in our cohort, as neither length of hospitalization nor duration of opioid treatment were associated with differences in CBCL scores. There continues to be a paucity of literature and mixed conclusions when examining associations between withdrawal severity and neurodevelopmental outcomes [4]. Previously, use of phenobarbital as adjunctive treatment for NOWS was shown to be associated with increased Internalizing and Total Problems on the CBCL, an effect thought to be related to either severity of NOWS or phenobarbital toxicity [12]. However, we found that neither the type of prenatal opioid exposure nor the specific treatment required for postnatal withdrawal was associated with increased risk of borderline/clinical range CBCL outcomes. This may suggest that the mechanism by which prenatal opioid exposure impacts risk for behavioral and emotional dysregulation is similar across different types of opioids, and the composite of social mechanisms associated with opioid use may have larger influence on outcomes than biological mechanisms specific to the opioid itself [13]. We note, however, that most of our cohort required pharmacologic treatment for NOWS. Future studies should include more children who did not require pharmacologic treatment to further delineate any associations between type of exposure or treatment for NOWS and risk for borderline/clinical CBCL outcomes.
Among the social risk factors we assessed, we identified discharge home with biological mother and a safety plan as a risk factor for borderline/clinical CBCL scores. Although discharge plans differ depending on the state or county workers involved, generally infants discharged home with their biological mother are considered to be in an environment with minimal psychosocial or physical risk. Infants discharged to foster care are discharged to an alternative environment with the goal of mitigating effects of active substance use by caregivers. Those who are discharged home with their biological mother and with a safety plan, however, are also considered to be entering an environment with some level of psychosocial risk. We hypothesize that this incompletely mitigated risk may contribute to slightly higher rates of behavioral and emotional problems in these children. Additionally, some of these children may have undergone custody status changes throughout the first two years of life, which was not explored in our analysis but may have still conferred risk compared to more stable environments. Others have also shown that the postnatal caregiving environment impacts outcomes. Children with prenatal opioid exposure who lived with foster or adoptive families had higher cognitive scores on the Bayley-III at age 2 years than those who lived with their biological parents [5]. In another study, children with prenatal heroin exposure raised by their biological parents had lower verbal IQ scores and learning abilities in math and reading, while children with prenatal heroin exposure who were adopted had normal verbal IQ scores and learning abilities in these domains [14]. Postnatal maternal psychological distress has been linked to increased Internalizing, Externalizing and Total Problems among children treated for NOWS [12]. While there are several confounding factors, the caregiving environment may impact childhood outcomes through various mechanisms. Further analysis including data on custody status at time of CBCL evaluation and number and type of custody status changes will be important for better understanding the association seen here.
Limitations of our study include its retrospective cohort design and selection bias in the cohort, as caregivers who maintained follow-up in our institution’s NOWS Clinic may have been those who perceived behavioral or emotional problems. Our cohort was large enough to detect associations between certain continuous variable risk factors (such as Bayley-III subscale scores) and CBCL outcomes, but small with respect to detecting associations between certain low-prevalence categorical risk factors and CBCL outcomes. We found that data on some socioeconomic covariates, like caregiver education, were not available for many of the children included in our cohort; however, we suspect that there may be additional associations between such covariates and borderline/clinical CBCL outcomes that we were unable to detect with our limited dataset. Given that our analysis included multiple comparisons which can potentially lead to chance findings, further investigation is warranted to confirm these findings.
Overall, this pilot study begins to highlight some important risk factors for various neurobehavioral outcomes among children with prenatal opioid exposure. Future studies with a larger sample size, including more equal representation of both children requiring and not requiring pharmacologic treatment, and with increased data on clinical and social variables that may be effect modifiers will deepen our understanding of the long-term outcomes of NOWS. Continued efforts towards a recovery-informed, non-stigmatizing evaluation of risk factors will help to engage both communities and providers to collaboratively identify potential target areas for intervention.
Data availability
The dataset generated for and analyzed during this study is available from the corresponding author upon reasonable request.
References
Arter SJ, Tyler B, McAllister J, Kiel E, Güler A, Cameron Hay M. Longitudinal Outcomes of Children Exposed to Opioids In‐utero: A Systematic Review. J Nurs Scholarsh. 2020;53:55–64.
Ornoy A, Segal J, Bar-Hamburger R, Greenbaum C. Developmental outcome of school-age children born to mothers with heroin dependency: importance of environmental factors. Dev Med Child Neurol. 2007;43:668–75.
Ornoy A, Daka L, Goldzweig G, Gil Y, Mjen L, Levit S, et al. Neurodevelopmental and psychological assessment of adolescents born to drug-addicted parents: Effects of SES and adoption. Child Abus Negl. 2010;34:354–68.
Conradt E, Flannery T, Aschner JL, Annett RD, Croen LA, Duarte CS, et al. Prenatal opioid exposure: neurodevelopmental consequences and future research priorities. Pediatrics. 2019;144:e20190128. https://doi.org/10.1542/peds.2019-0128.
Merhar SL, McAllister JM, Wedig-Stevie KE, Klein AC, Meinzen-Derr J, Poindexter BB. Retrospective review of neurodevelopmental outcomes in infants treated for neonatal abstinence syndrome. J Perinatol. 2018;38:587–92.
Achenbach TM, Rescorla LA. Manual for the ASEBA preschool forms and profiles: An integrated system of multi-informant assessment. Burlington, VT: ASEBA; 2010.
Comprehensive Assessment Planning Model Safety Plan for Children Instructions. In: E-Manuals JFS. https://emanuals.jfs.ohio.gov/pdf/pdf-letters/FCASMTL-522----Safety-Plan-Forms.pdf.
de Cubas MM, Field T. Children of methadone-dependent women: developmental outcomes. Am J Orthopsychiatr. 1993;63:266–76. https://doi.org/10.1037/h0079429.
Beckwith AM, Burke SA. Identification of early developmental deficits in infants with prenatal heroin, methadone, and other opioid exposure. Clin Pediatr (Philos). 2015;54:328–35. https://doi.org/10.1177/0009922814549545.
Hunt RW, Tzioumi D, Collins E, Jeffery HE. Adverse neurodevelopmental outcome of infants exposed to opiate in-utero. Early Hum Dev. 2008;84:29–35. https://doi.org/10.1016/j.earlhumdev.2007.01.013.
van Baar AL, Soepatmi S, Gunning WB, Akkerhuis GW. Development after prenatal exposure to cocaine, heroin and methadone. Acta Paediatr Suppl. 1994;404:40–6. https://doi.org/10.1111/j.1651-2227.1994.tb13383.x.
Czynski AJ, Davis JM, Dansereau LM, Engelhardt B, Marro P, Bogen DL, et al. Neurodevelopmental outcomes of neonates randomized to morphine or methadone for treatment of neonatal abstinence syndrome. J Pediatr. 2020;219:146–51.e1.
Conradt E, Camerota M, Maylott S, Lester BM. Annual Research Review: Prenatal opioid exposure - a two-generation approach to conceptualizing neurodevelopmental outcomes. J Child Psychol Psychiatry. 2023;64:566–78.
Ornoy A, Segal J, Bar-Hamburger R, Greenbaum C. Developmental outcome of school-age children born to mothers with heroin dependency: importance of environmental factors. Dev Med Child Neurol. 2001;43:668–75.
Acknowledgements
We are grateful to the patients and families seen in our NOWS clinic for their involvement in this study. The authors have no sources of funding relevant to this study to report.
Author information
Authors and Affiliations
Contributions
J. McAllister and S. Merhar conceptualized the study and its methods. N. Baig and J. McAllister performed data collection. S. Ehrlich, C. Liu, and Q. Sun performed the data analyses, assisted with preparation of the included tables, and reviewed the manuscript. The manuscript was prepared by all the included authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Baig, N., Sun, Q., Liu, C. et al. Neurobehavioral problems at age 2 years in children with prenatal opioid exposure. J Perinatol (2024). https://doi.org/10.1038/s41372-024-01913-7
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41372-024-01913-7
