
Abstract
The association between childhood bullying victimisation and mental health problems in adulthood has been consistently reported in the literature. Previous studies used both retrospective and prospective reports to measure bullying victimisation. However, there could be biases in both reports. We aimed to assess agreement between prospective and retrospective reports of childhood bullying victimisation, to compare their associations with mental health in early adulthood, and to examine the associations of consistent prospectively and retrospectively reported bullying victimisation with adult mental health. Data were from the prospective Bavarian Longitudinal Study of neonatal at-risk children and term-born controls recruited at birth. 489 participants were followed from birth to age 26 (mean [SD]: 26.4 [0.8] years). Adult mental health was assessed using both the Achenbach Young Adult Self-Report (YSR) and standardised diagnostic interviews. Childhood bullying victimisation was prospectively reported by participants and parents at age 13 and retrospectively self-reported at age 26. We showed that the agreement between retrospective and prospective self-reports of bullying victimisation was fair (Kappa 0.30) with only slight agreement (Kappa 0.18) when compared with prospective parent-reports. Both prospectively and retrospectively self-reported bullying victimisation was associated with poor mental health. Retrospective reports tended to produce stronger associations. Participants who reported being bullied both retrospectively and prospectively had a particularly elevated risk for mental health problems. In conclusion, prospective and retrospective reports capture partly different individuals with exposure to bullying victimisation. Exposure to bullying victimisation, whether it was retrospectively or prospectively self-reported, was associated with an increased risk for mental health problems.
Similar content being viewed by others


Introduction
Bullying involves intentional and repeated acts of aggression over time with an imbalance of power (Olweus, 1994). Based on nationally-representative data from 71 countries in 2018, 30% of children globally experienced frequent victimisation and over 20% in European countries (Hosozawa et al., 2021). Bullying can be physical, verbal, or relational with the first two forms labelled as “direct bullying” as they include direct aggressive acts such as hitting, kicking, or direct verbal abuse. In contrast, relational bullying refers to social exclusion by spreading malicious gossip or withdrawal of friendship (Woods & Wolke, 2004). The association between childhood bullying victimisation and adult mental health problems (e.g., general mental well-being, depression, anxiety, delinquent behaviour) has been consistently reported in the literature (Armitage et al., 2021a; Copeland et al., 2013; Kehusmaa et al., 2022; Wolke & Lereya, 2015).
Despite increasing longitudinal studies on bullying victimisation and adult mental health recently, many studies have relied on adults’ recollections of childhood experiences (Wolke & Lereya, 2015), which is less time consuming and expensive than prospective longitudinal studies. However, retrospective reports of bullying victimisation share the same limitations as those of adverse childhood experiences (ACEs), for instance, the influence of memory loss, distortion and subsequent life experiences and limitations regarding causal inferences (Hardt & Rutter, 2004; Tajima et al., 2004), thus raising concerns regarding the validity of retrospective reports. A further limitation relates to the misclassification of the exposure status due to measurement errors from inaccurate recall. This, from an epidemiological perspective, can introduce bias in the associations between the exposure and outcomes of interest and lead to differential misclassification. One scenario is that the presence of mental health problems in adulthood may unconsciously increase an individual’s tendency to recall childhood bullying victimisation. This can be called false positive classification (Bower, 1981) and is regarded as one type of differential misclassification (Pearce et al., 2007). It might inflate the association between early experience and mental health. Another scenario is that individuals in good circumstances in adulthood may be more likely to forget early bullying victimisation or reconstruct happier childhoods. It can be called false negative classification, another type of differential misclassification (Hardt & Rutter, 2004; Maughan et al., 1995; Robins et al., 1985), also leading to an overestimated association with mental health (Hardt & Rutter, 2004; Patten et al., 2015).
Childhood bullying victimisation has also been measured prospectively in longitudinal studies (Armitage et al., 2021a; Copeland et al., 2013; Kehusmaa et al., 2022; Lereya et al., 2015a, b), such as child self-reports and parent-reports at the time that the events occurred. Longitudinal research offers the opportunity to identify the temporal sequencing of events critical to establish causality but selective drop-out often associated with social disadvantage could lead to selection bias and limit the generalisability of research findings. There is also potential for under-reports depending on informant, e.g., parents may be unaware of incidences of bullying, especially relational bullying that is less observable (Ronning et al., 2009).
Previous studies of ACEs examined the reliability of retrospective and prospective reports using a test–retest paradigm and looking at the concordance or corroboration between two measures on two occasions (Baldwin et al., 2019). A meta-analysis of 16 studies showed only slight agreement (Kappa 0.19) between prospective and retrospective measures (Baldwin et al., 2019). Studies that further compared their associations with mental health showed that retrospective self-reports tend to demonstrate stronger associations with mental health problems involving an affective component including depression (Newbury et al., 2018; Patten et al., 2015; Tajima et al., 2004). For instance, Patten et al. (2015) showed that the elevated odds for major depressive episode were over 2.5 times greater for childhood adversity assessed retrospectively in adulthood compared to prospective reports, but this pattern was absent for alcohol use and other outcomes. Similar patterns were reported in other studies (Newbury et al., 2018). Furthermore, two studies reported the highest rates of problem behaviours in individuals reporting ACEs both prospectively and retrospectively (Tajima et al., 2004; Widom et al., 1999). No study has yet compared prospective and retrospective reports of bullying.
It is uncertain whether the findings from child maltreatment would be similar or different for bullying victimisation. Bullying and ACEs share similarities in their effects on adult mental health (Croft et al., 2019). However, some evidence suggests that being bullied might have similar or even worse long-term adverse effects than being maltreated (Lereya et al., 2015a, 2015b). Bullying might also differ from child maltreatment in that peer bullying tends to occur most frequently at school age while over half of maltreatment of children occurs in the age range of birth through 3 years old (U.S. Department of Health & Human Services, 2023). Thus bullied children are thought to have the capacity to better understand what is happening to them (Widom, 2020) and this may contribute to potentially improved retrospective recall of the event in adulthood.
Further, as explained earlier, two types of differential misclassification exist in retrospective recall of ACEs which could potentially introduce a bias in the associations between bullying victimisation and mental health. More research is needed to clarify the direction of the recall bias, for instance, whether there is over reporting of childhood bullying victimisation among individuals with poor adult life situations (e.g., poor life satisfaction or mental health) and underreporting among those in good circumstances (e.g., high adult life satisfaction or mental health).
In this study, we assess agreement between prospective and retrospective reports of childhood bullying victimisation (i.e., whether the two measures identify the same individuals) and compare their associations with mental health in early adulthood. We hypothesise a low agreement between prospective and retrospective reports and that retrospective reports would have stronger associations with adult mental health based on previous studies on child maltreatment. We also examine the associations of consistent prospectively and retrospectively reported bullying victimisation with adult mental health and hypothesise that such consistent victimisation report would have stronger associations. Moreover, we explore whether any retrospective recall bias may be related to concurrent life satisfaction or mental health in adulthood by comparing the agreement between prospective and retrospective reports of bullying victimisation according to current life satisfaction or mental health, for instance, whether there is over reporting of childhood bullying victimisation among individuals with poor adult life satisfaction or mental health and underreporting among those with high adult life satisfaction or mental health.
Methods
Participants
We performed a secondary data analysis using data collected from the prospective Bavarian Longitudinal Study (BLS), a geographically defined whole-population sample of neonatal at-risk and healthy children born between January 1985 and March 1986 in Southern Bavaria, Germany. The enrolment and data collection procedures for the BLS have been described in detail elsewhere (Wolke & Meyer, 1999). In brief, the BLS assesses an entire population sample of 682 individuals born very preterm (VP; < 32 weeks of gestation) and/or very low birth weight (VLBW; birthweight < 1500 g) and matched comparison participants born at term. Participants were followed up at birth, 5, 20 and 56 months of age, 6, 8 and 13 years, and again at 26 years. Of the 682 VP/VLBW infants recruited at birth, 448 were alive and eligible for inclusion at age 13, and 339 (84%) were assessed. At age 26, 260 (63.3%) of 411 eligible participants (alive, living in Germany) were assessed. Of 916 healthy term-born children in the same hospitals during the same period, who received normal postnatal care, 350 survivors were selected to be comparable to the overall distribution of child sex, family socioeconomic status (SES), and maternal age of the VP/VLBW group. At age 13, 350 participants were eligible and 293 (84%) were assessed. At age 26, 308 participants were eligible and 229 (74.4%) were assessed.
Initial ethical approval was obtained from the Ethics Committee of the University of Munich Children’s Hospital and the Bavarian Health Council. Ethical approval for the follow-up in adulthood was obtained from the Ethical Board of the University Hospital Bonn (reference 159/09). Parents provided informed written consent within 48 h of their child’s birth and all adult participants provided informed written consent. For adult participants with severe impairment, consent was provided by an assigned guardian.
Measures
Prospective reports of bullying victimisation
At 13 years, this was reported by parents and children using one item of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 2001): “other children pick on or bully him/her” (parent reports) or “other children pick on or bully me” (self-reports). Response options included “certainly true”, “somewhat true”, and “not true”. Answers of “certainly true” or “somewhat true” were considered as bullying victimisation (yes versus no).
Retrospective reports of bullying victimisation
At age 26, participants retrospectively self-reported on their childhood experience of bullying victimisation through a life-course interview. Participants were asked to complete unseen by the interviewer a structured questionnaire of bullying during childhood comprising nine items adapted from previous research (Wolke et al., 2000) for retrospective questioning in adulthood (Lin et al., 2020; Wolke & Sapouna, 2008). Two types of bullying were captured: direct and relational. Items for direct bullying included: (1) having been beaten or pushed around; (2) having belongings stolen or deliberately destroyed; (3) having been physically threatened or blackmailed; (4) having pranks played on them; and (5) having been verbally abused or insulted. Items for relational bullying included: (1) having lies or rumours told about them; (2) having been deliberately ignored or neglected; (3) having been deliberately not invited to play or parties; and (4) having been harassed in other ways. Participants indicated the frequency of each item during school days (never; once or twice; two or three times per month; once or several times per week). Answers of ‘two or three times per month’ or more often to any item were considered as bullying victimisation (yes versus no) based on the definition of bullying which stressed ‘repeated acts of aggression’. This approach has been used previously (Lereya et al., 2013). Cronbach’s Alpha of the nine items was 0.88 in the current sample.
Based on prospective and retrospective self-reports, experience of bullying victimisation was coded into four categories: 4 = bullying victimisation reported both prospectively and retrospectively (consistent reports), 3 = bullying victimisation only reported retrospectively, 2 = bullying victimisation only reported prospectively, and 1 = no bullying victimisation from both reports. This variable was created to examine the associations of consistent prospectively and retrospectively reported bullying victimisation with adult mental health.
Adult life satisfaction
This was measured using the five-item Satisfaction with Life Scale (SWLS) (Diener et al., 1985), which has favourable psychometric properties and is suitable for different age groups (Diener et al., 1985). The five items include: (1) in most ways my life is close to ideal; (2) the conditions of my life are excellent; (3) I am satisfied with my life; (4) so far, I have gotten the important things I want in life; and (5) if I could live my life over, I would change almost nothing. Each item is measured on a 7-point scale from 1 = strongly disagree to 7 = strongly agree. A total score was calculated by summing up scores of all items, ranging from 5 (low satisfaction) to 35 (high). Participants were considered to have high life satisfaction if they scored ≥ 25 and average or low satisfaction if scored ≤ 24 (Diener, 2006). Cronbach’s alpha for this scale in this sample was 0.87.
Adult mental health
It was assessed using the Achenbach Young Adult Self-Report (YASR) (Achenbach, 1997) completed by participants at the 26-year assessment between 2011 and 2013. The YASR is a standardised instrument used to assess behavioural and emotional problems. It has an initial 116 items where participants answer whether a statement is not true (0), somewhat or sometimes true (1) or very true (2). Scores for all subscales were calculated by summing the score on each respective question. Scores of the subscales ‘anxious/depressed’ (17 items) and ‘withdrawn’ (7 items) were further combined into internalising problems, while scores of the subscales ‘aggressive behaviour’ (12 items), ‘rule-breaking behaviour’ (9 items), and ‘intrusive behaviour’ (7 items) were combined into externalising problems (supplementary Table S1).
Psychiatric disorder diagnoses were also obtained at age 26 years using a computer-assisted version of the Munich Composite International Diagnostic Interview according to DSM-IV criteria (DIA-X/M-CIDI). This has been previously described (Jaekel et al., 2018). We assessed the presence of mood disorder, anxiety disorder, substance abuse, and any eating disorder. For this study, we focused on any anxiety disorder (yes versus no) and any mood disorder (yes versus no), as well as any psychiatric disorder (defined as having any of the above disorders assessed, yes versus no). The M-CIDI has good diagnostic agreement compared with clinical diagnoses (Kappa = 0.50–0.96) (Reed et al., 1998) and good concordance with the Structured Clinical Interview for DSM-IV (Haro et al., 2006).
Confounders
The choice of confounders was based on previous research (Analitis et al., 2009; Wolke et al., 2015), including sex assigned at birth (male versus female), family SES at birth (low, moderate or high; supplementary materials), and pre-existing total emotional and behavioural problems at age 6. Pre-existing total emotional and behavioural problems at age 6 was assessed using the German version of the Child Behaviour Checklist (CBCL) at age 6 years. The CBCL is a parent-report measure designed to assess a wide range of behavioural and emotional problems in children. It is comprised of 106 items, each rated on a 3-point scale (“not true”, “somewhat true” and “always or often true”). Parents were instructed to rate each item based on the participants’ presentation in the last 6 months. Cronbach’s alpha for the overall scale was 0.91.
Data analysis
Analyses were conducted in STATA 16.0. We first calculated the agreement between prospective and retrospective self-reports of bullying victimisation using Cohen's Kappa. Kappa values of 0.00–0.20 are considered as having slight agreement, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement (Landis & Koch, 1977). Prospective parent-reports and retrospective self-reports were also compared. A sensitivity analysis was performed using a different cut-off (once or twice) for retrospective reports. We then used Tobit model to estimate the associations of bullying victimisation with continuous outcomes (i.e., scores of internalising and externalising symptoms) and logistic regression for binary outcomes (i.e., the presence of mental disorder). Tobit model, also called a censored regression model, was used given the left- and right-censoring in the dependent variables. Effect sizes were measured using mean differences and 95% confidence intervals (CIs) for continuous outcomes and odds ratios (ORs) for binary outcomes. In all models, we adjusted for sex, family SES, and pre-existing emotional and behavioural problems. Differences in bullying between participants born VP/VLBW and controls were reported previously (Wolke et al., 2015). The two groups were analysed as a combined sample and then analysed separately as a sensitivity analysis (supplementary Tables S3 and S4). As results are similar, only those from the combined sample are reported in the main text. Among 632 participants assessed at 13 years, 459 were assessed at 26 years. We performed a drop-out analysis to compare those assessed and not assessed at 26 years (supplementary Table S5) which indicated a lower proportion of low/moderate SES in the assessed participants at age 26, a lower proportion of participants with bullying victimisation at age 13, and less pre-existing emotional and behavioural problems at age 6. Multiple imputation was applied to account for both drop-out and missing data (supplementary Tables S6 and S7), which did not alter the key findings. Imputation models included variables on bullying victimisation, outcome variables, and other confounders (i.e., sex, family SES, pre-existing total emotional and behavioural problems). Finally, to explore retrospective recall bias associated with current life satisfaction or mental health, we followed the same strategy used by Maughan et al. (1995) and performed a stratification analysis of examining agreement between prospective and retrospective self-reports of victimisation by life satisfaction (average or low versus high) or diagnosis of psychiatric disorder (yes versus no). Taking prospective reports as the criterion, sensitivity (true positive rate) and specificity (true negative rate) were calculated. Sensitivity measures the proportion of positives that were prospectively identified, while specificity (true negative rate) measures the proportion of negatives that were prospectively identified.
Results
Agreement between prospective and retrospective reports
In total, 424 participants had available data on bullying victimisation for both prospective parent-reports and retrospective self-reports; 416 participants had available data for both prospective self-reports and retrospective self-reports (Table 1). Prospective-retrospective Kappa agreement was slight when comparing across-source reports (child-parent: Kappa 0.18) and fair when using the same source (self-report: Kappa 0.30). There was fair to moderate agreement between parent-reports and self-reports at 13 years (Kappa 0.39). Of 416 participants with data on both prospective and retrospective self-reports, 30.1% prospectively reported bullying victimisation at 13 years, while 28.6% retrospectively reported such experience at 26 years (direct: 26.1%; relational: 17.9%). When using a different cut-off (once or twice), the prevalence of bullying victimisation for retrospective reports increased to 43.1% but Kappa agreement showed similar results (supplementary Table S2).
Associations of bullying victimisation with adult mental health
Among 489 participants assessed at 26 years, 460 had data on self-reported internalising symptoms and 486 had data on mental disorders. Of 486 participants, 98 (19.8%) and 125 (25.7%) had diagnoses of mood disorder and anxiety disorder, respectively. Childhood bullying victimisation was associated with an increased risk of internalising and externalising problems in adulthood, with almost all associations reaching significance (mean differences ranging from 2.02–5.29; Table 2) except for the association between prospectively parent-reported bullying victimisation and externalising problems. Both prospective and retrospective self-reports of childhood bullying victimisation, but not prospective parent-reports, were associated with elevated diagnoses of mood disorder, anxiety disorder and total psychiatric disorder (ORs ranging from 1.74–3.60; Table 2). When comparing effect size differences between prospective and retrospective self-reports, despite overlapping confidence intervals, retrospective reports tended to produce stronger associations with mental health problems except for externalising problems (Table 2).
Consistent reports of bullying victimisation and adult mental health
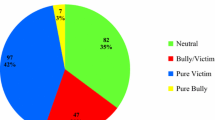
Among 416 participants with data on prospective and retrospective self-reports of bullying victimisation, 14.9% (n = 62) both prospectively and retrospectively reported to have experienced bullying victimisation in childhood, 13.7% (n = 57) only retrospectively reported such experience, and 15.1% (n = 63) only prospectively reported victimisation.
Relative to participants with neither prospective nor retrospective reports of bullying victimisation, those with consistent self-reports were at increased risk for both self-reported internalising and externalising problems and psychiatric diagnosis in adulthood. These associations were stronger compared with bullying victimisation only reported retrospectively (Table 3). For instance, the effect size was over two times higher for self-reported internalising problems (mean difference 7.94 versus 3.74) and the diagnosis of any psychiatric disorder (OR: 4.00 versus 2.44). Bullying victimisation, if only reported prospectively, was only associated with externalising problems (Table 3).
Exploratory analysis of bias in retrospective recall
As reflected in sensitivity and Kappa agreement (Table 4), different patterns were found in the agreement between prospective and retrospective reports of bullying victimisation according to whether the participants had high life satisfaction or good mental health (without psychiatric disorder) in adulthood. Kappa value was lower for participants with high life satisfaction (0.24) than those having average or low life satisfaction (0.43), but the difference was not statistically significant as indicated by overlapping confidence intervals. More prospectively identified cases failed to be identified in retrospective reports for participants with high life satisfaction, resulting in a lower sensitivity than those with low life satisfaction (0.41 versus 0.75). The stratification analysis by psychiatric disorder showed similar results (Table 4). Thus, it appears unlikely for participants with low life satisfaction or poor mental health to over report childhood bullying victimisation. As indicated by the low sensitivity and agreement, there might be a tendency for those with high life satisfaction and good mental health in adulthood to under report childhood bullying victimisation.
Discussion
To our knowledge, this is the first longitudinal study comparing prospective and retrospective reports of childhood bullying victimisation in relation to mental health in adulthood. We found slight to fair agreement between the two types of reports. Both prospectively and retrospectively self-reported childhood bullying victimisation were associated with mental health in early adulthood with retrospective self-reports having the tendency for stronger associations. Participants who consistently reported being bullied based on both prospective reports at 13 years and retrospective reports at 26 years had a particularly elevated risk for poor mental health.
Our analysis showed only a slight to fair agreement between prospective and retrospective reports of childhood bullying victimisation, consistent with studies of child maltreatment (Baldwin et al., 2019). It could be due to differences between prospective and retrospective measures of childhood bullying victimisation, e.g., response option, report source (prospective parent-reports vs retrospective self-reports), number of questions used (one general item at age 13 versus a range of specific behaviours at age 26) or reporting period (past six months versus the whole of the school years). Additionally, despite the use of a structured questionnaire at age 26, there is still potential for underestimates due to issues such as poor memory or denial in adulthood, which may have reduced the agreement between prospective and retrospective reports. However, retrospectively bullying victimisation was obtained in early adulthood. This may help to reduce the time in which childhood memories might be forgotten (Newbury et al., 2018). Considering the above differences, the agreement in self-reports of Kappa 0.30 is higher compared with other ACEs. Furthermore, as pointed out by Baldwin et al. (2019), the low agreement between prospective and retrospective measures of ACEs cannot be interpreted to directly indicate poor validity of retrospective measures. When ACEs are retrospectively reported to have occurred, these reports are likely to be correct (Hardt & Rutter, 2004). Bullying victimisation only reported retrospectively could be what was missed in the prospective reports (e.g., had occurred in elementary school or after the 13-year assessment in secondary school) rather than measurement errors in the memories looking back. Our findings suggest that prospective and retrospective reports of childhood bullying victimisation identify partly different groups of individuals and, thus, cannot be used interchangeably, aligned with research in child maltreatment (Baldwin et al., 2019).
The Kappa value was lower when comparing prospective parent-reports to retrospective self-reports, which is unsurprising given the only fair agreement of reports by parents and children as indicated both in our study and previously (Copeland et al., 2013; Ronning et al., 2009) with parents less aware of school bullying victimisation, especially relational bullying. Our finding indicates the value of using multiple informants in future research to get a more accurate measure of bullying experiences and robust estimates of victimisation outcomes (Armitage et al., 2022). Both prospectively and retrospectively self-reported childhood bullying victimisation were associated with self-reported mental health and psychiatric diagnoses at age 26. There was, however, a difference regarding prospective parent-reports in that there were no significant associations with psychiatric diagnoses, suggesting that parent-reports might not be as valid as self-reports when examining the long-term effects of bullying victimisation. This could be due to the shared rater effect whereby bullying victimisation and mental health were reported by the same rater which may have increased the likelihood of an association (Schoeler et al., 2018). It could also be that parent-reports capture a different picture of bullying experience compared to self-reports, for instance, more physical experiences that are more observable. Physical forms of bullying victimisation may be less strongly associated with mental health than relational experiences (Wolke & Lereya, 2015).
Furthermore, we show that retrospective self-reports had the tendency to produce stronger associations with mental health problems, a pattern consistent with prior literature regarding childhood adversities (Newbury et al., 2018; Patten et al., 2015; Tajima et al., 2004). It may be that young adults with adverse current outcomes tend to remember more negative versus positive childhood experiences because of their current mood, which can be termed as false positive differential misclassification, as explained in the introduction. This is the bias that has been usually assumed, but it does not seem to be supported by our and previous research findings (Fergusson et al., 2000; Paivio, 2001). Our exploratory analysis suggests the unlikelihood of participants with low life satisfaction or poor mental health in adulthood to over report childhood bullying victimisation. A more likely explanation relates to false negative differential misclassification in the retrospective reports among individuals with positive outcomes in adult life. Our analysis suggests that there might be a tendency for those with current high life satisfaction or good mental health in adulthood to under report childhood bullying victimisation, compared with those with adverse adult outcomes. This is in line with Maughan et al. (1995) and Robins et al. (1985) and a recent study looking into positive wellbeing and resilience following adolescent victimisation (Armitage et al., 2021b). This false negative differential misclassification may lead to the inflated associations between retrospective reports of bullying victimisation and mental health (Patten et al., 2015). Furthermore, it is possible that many cases of bullying victimisation were not reported prospectively at age 13, which might have slightly reduced the associations of prospective reports with mental health.
Notably, retrospective self-reports (versus prospective self-reports) only had stronger associations with mental health problems that are inner-directed and contain an affective component (Forns et al., 2011) (e.g., depression, anxiety, and withdrawal). In contrast, this differential association was absent for externalising problems that are outer-directed and involve a behavioural domain (Forns et al., 2011) (e.g., impulsivity, aggressiveness, and disruptiveness). These findings parallel results from studies of child maltreatment (Newbury et al., 2018), possibly explained by the non-differential recall misclassification in certain circumstances (Patten et al., 2015). That is, in the case of externalising problems, differential recall might not occur in the way that affective forms of psychopathology may be. In other words, retrospective misclassification of bullying victimisation may be non-differential with respect to adult externalising problems.
Finally, participants who consistently reported being bullied had a particularly elevated risk for poor mental health, following the same pattern reported by Tajima et al. (2004) and Widom et al. (1999). There was a slight difference in the prevalence rates (e.g., 15% reported on both prospective and retrospective bullying victimisation and around 14–15% reported one measure). Yet there appeared to be a substantial difference in the risk of mental health problems. The stronger association for consistent reports with mental health could be inflated due to the use of different items retrospectively and prospectively or the fact that retrospective reports and the outcomes were measured at the same time. However, it could also be a genuine finding. If participants report bullying victimisation both prospectively and retrospectively, it may be that such experience is harder to forget and can be used as an indication of severity of victimisation.
There are several limitations. First, there were differences between prospective and retrospective measures of childhood bullying victimisation, e.g., number of questions (one general item from SDQ at age 13 versus a range of specific items at age 26) and reporting period (past six months versus the whole of the school years), which may have led to under-reporting in childhood. There was also no clear definition of bullying provided at age 13, so participants might have different interpretations of bullying. However, our rate of bullying victimisation reported at age 13 was not different from national estimates in Germany during a similar time period (boys 39%; girls 32%) (Due et al., 2008). Second, differences in the degree and type of bullying victimisation between prospective and retrospective reports were not compared due to the use of different instruments and response options. In retrospective reports, participants indicated the frequency of each item occurred and the measure covered both direct and relational experiences, while only one general item was used in prospective reports and with different response options. These can potentially influence the strength of the association between victimisation and mental health. Future research should build on our study by increasing the comparability of the measurement at both time points. Lastly, due to the small sample size, we were not able to explore sex differences in the association between bullying victimisation and mental health. Further, given overlapping confidence intervals, our study might be underpowered to properly test the biases on retrospective recall Our study need to be replicated in studies with large sample sizes. Nevertheless, we used multiple imputation to deal with drop-out and missing data to minimise data loss which have strengthened our findings on the association analysis.
Conclusion
Our results support that prospective and retrospective reports of bullying victimisation hold value in research as they could capture different individuals who were exposed to bullying victimisation and the use of both could potentially reduce false negative classification in bullying victimisation. Exposure to bullying victimisation, whether it was retrospectively or prospectively self-reported, was associated with an increased risk for mental health problems in early adulthood. Retrospective reports tended to have stronger associations with affective forms of mental health. Given the high prevalence of bullying and its long-term mental health consequences, more effective anti-bullying interventions are needed to reduce childhood bullying, in order to improve current and long-term mental health in children and adolescents.
Data availability
Data could be obtained upon request.
References
Achenbach, T. M. (1997). Manual for the young adult self-report and young adult behavior checklist. University of Vermont.
Analitis, F., Velderman, M. K., Ravens-Sieberer, U., Detmar, S., Erhart, M., Herdman, M., ... & European Kidscreen Group. (2009). Being bullied: associated factors in children and adolescents 8 to 18 years old in 11 European countries. Pediatrics, 123(2), 569-577.
Armitage, J. M., Morneau‐Vaillancourt, G., Pingault, J., Andlauer, T. F. M., Paquin, S., Langevin, S., Brendgen, M., Dionne, G., Séguin, J. R., Rouleau, G., Vitaro, F., Ouellet‐Morin, I., & Boivin, M. (2022). A multi‐informant and multi‐polygenic approach to understanding predictors of peer victimisation in childhood and adolescence. JCPP Advances, 2(1). https://doi.org/10.1002/jcv2.12063
Armitage, J. M., Wang, R. A., Davis, O. S., Bowes, L., & Haworth, C. M. (2021a). Peer victimisation during adolescence and its impact on wellbeing in adulthood: A prospective cohort study. BMC Public Health, 21(1), 148. https://doi.org/10.1186/s12889-021-10198-w
Armitage, J. M., Wang, R. A., Davis, O. S., Collard, P., & Haworth, C. M. (2021b). Positive wellbeing and resilience following adolescent victimisation: An exploration into protective factors across development. JCPP Advances, 1(2), e12024.
Baldwin, J. R., Reuben, A., Newbury, J. B., & Danese, A. (2019). Agreement between prospective and retrospective measures of childhood maltreatment: A systematic review and meta-analysis. JAMA Psychiatry, 76(6), 584–593. https://doi.org/10.1001/jamapsychiatry.2019.0097
Bower, G. H. (1981). Mood and memory. American Psychologist, 36(2), 129–148. https://doi.org/10.1037//0003-066x.36.2.129
Copeland, W. E., Wolke, D., Angold, A., & Costello, E. J. (2013). Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry, 70(4), 419–426. https://doi.org/10.1001/jamapsychiatry.2013.504
Croft, J., Heron, J., Teufel, C., Cannon, M., Wolke, D., Thompson, A., Houtepen, L., & Zammit, S. (2019). Association of trauma type, age of exposure, and frequency in childhood and adolescence with psychotic experiences in early adulthood. JAMA Psychiatry, 76(1), 79–86. https://doi.org/10.1001/jamapsychiatry.2018.3155
Diener, E. (2006). Understanding the SWLS scores. http://labs.psychology.illinois.edu/~ediener/Documents/Understanding%20SWLS%20Scores.pdf. Accessed 26 Feb 2024
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s15327752jpa4901_13
Due, P., Holstein, B. E., & Soc, M. S. (2008). Bullying victimization among 13 to 15-year-old school children: Results from two comparative studies in 66 countries and regions. International Journal of Adolescent Medicine and Health, 20(2), 209–221. https://doi.org/10.1515/ijamh.2008.20.2.209
Fergusson, D. M., Horwood, L. J., & Woodward, L. J. (2000). The stability of child abuse reports: A longitudinal study of the reporting behaviour of young adults. Psychological Medicine, 30(3), 529–544. https://doi.org/10.1017/s0033291799002111
Forns, M., Abad, J., & Kirchner, T. (2011). Internalizing and Externalizing Problems. In R. J. R. Levesque (Ed.), Encyclopedia of Adolescence (pp. 1464–1469). Springer New York. https://doi.org/10.1007/978-1-4419-1695-2_261
Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry, 40(11), 1337–1345. https://doi.org/10.1097/00004583-200111000-00015
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. https://doi.org/10.1111/j.1469-7610.2004.00218.x
Haro, J. M., Arbabzadeh-Bouchez, S., Brugha, T. S., de Girolamo, G., Guyer, M. E., Jin, R., Lepine, J. P., Mazzi, F., Reneses, B., Vilagut, G., Sampson, N. A., & Kessler, R. C. (2006). Concordance of the composite international diagnostic interview version 3.0 (CIDI 3.0) with standardized clinical assessments in the WHO world mental health surveys. International Journal of Methods in Psychiatric Research, 15(4), 167–180. https://doi.org/10.1002/mpr.196
Hosozawa, M., Bann, D., Fink, E., Elsden, E., Baba, S., Iso, H., & Patalay, P. (2021). Bullying victimisation in adolescence: Prevalence and inequalities by gender, socioeconomic status and academic performance across 71 countries. EClinicalMedicine, 41, 101142. https://doi.org/10.1016/j.eclinm.2021.101142
Jaekel, J., Baumann, N., Bartmann, P., & Wolke, D. (2018). Mood and anxiety disorders in very preterm/very low-birth weight individuals from 6 to 26 years. Journal of Child Psychology and Psychiatry and Allied Disciplines, 59(1), 88–95. https://doi.org/10.1111/jcpp.12787
Kehusmaa, J., Ruotsalainen, H., Männikkö, N., Alakokkare, A. E., Niemelä, M., Jääskeläinen, E., & Miettunen, J. (2022). The association between the social environment of childhood and adolescence and depression in young adulthood - A prospective cohort study. Journal of Affective Disorders, 305, 37–46. https://doi.org/10.1016/j.jad.2022.02.067
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), 159–174. https://www.ncbi.nlm.nih.gov/pubmed/843571. Accessed 26 Feb 2024
Lereya, S. T., Copeland, W. E., Costello, E. J., & Wolke, D. (2015a). Adult mental health consequences of peer bullying and maltreatment in childhood: Two cohorts in two countries. Lancet Psychiatry, 2(6), 524–531. https://doi.org/10.1016/S2215-0366(15)00165-0
Lereya, S. T., Copeland, W. E., Zammit, S., & Wolke, D. (2015b). Bully/victims: A longitudinal, population-based cohort study of their mental health. European Child & Adolescent Psychiatry, 24(12), 1461–1471. https://doi.org/10.1007/s00787-015-0705-5
Lereya, S. T., Winsper, C., Heron, J., Lewis, G., Gunnell, D., Fisher, H. L., & Wolke, D. (2013). Being bullied during childhood and the prospective pathways to self-harm in late adolescence. Journal of the American Academy of Child & Adolescent Psychiatry, 52(6), 608–618.
Lin, M., Wolke, D., Schneider, S., & Margraf, J. (2020). Bullies get away with it, but not everywhere: Mental health sequelae of bullying in Chinese and German students. Journal of Cross-Cultural Psychology, 51(9), 702–718. https://doi.org/10.1177/0022022120949913
Maughan, B., Pickles, A., & Quinton, D. (1995). Parental hostility, childhood behavior, and adult social functioning. In J. McCord (Ed.), Coercion and Punishment in Long-Term Perspectives (pp. 34–58). Cambridge University Press. https://doi.org/10.1017/CBO9780511527906.003
Newbury, J. B., Arseneault, L., Moffitt, T. E., Caspi, A., Danese, A., Baldwin, J. R., & Fisher, H. L. (2018). Measuring childhood maltreatment to predict early-adult psychopathology: Comparison of prospective informant-reports and retrospective self-reports. Journal of Psychiatric Research, 96, 57–64. https://doi.org/10.1016/j.jpsychires.2017.09.020
Olweus, D. (1994). Bullying at school. In L. R. Huesmann (Ed.), Aggressive Behavior (pp. 97–130). Springer. https://doi.org/10.1007/978-1-4757-9116-7_5
Paivio, S. C. (2001). Stability of retrospective self-reports of child abuse and neglect before and after therapy for child abuse issues. Child Abuse & Neglect, 25(8), 1053–1068. https://doi.org/10.1016/s0145-2134(01)00256-3
Patten, S. B., Wilkes, T. C., Williams, J. V., Lavorato, D. H., El-Guebaly, N., Schopflocher, D., Wild, C., Colman, I., & Bulloch, A. G. (2015). Retrospective and prospectively assessed childhood adversity in association with major depression, alcohol consumption and painful conditions. Epidemiology and Psychiatric Sciences, 24(2), 158–165. https://doi.org/10.1017/S2045796014000018
Pearce, N., Checkoway, H., & Kriebel, D. (2007). Bias in occupational epidemiology studies. Occupational and Environmental Medicine, 64(8), 562–568. https://doi.org/10.1136/oem.2006.026690
Reed, V., Gander, F., Pfister, H., Steiger, A., Sonntag, H., Trenkwalder, C., Sonntag, A., Hundt, W., & Wittchen, H.-U. (1998). To what degree does the Composite International Diagnostic Interview (CIDI) correctly identify DSM-IV disorders? Testing validity issues in a clinical sample. International Journal of Methods in Psychiatric Research, 7(3), 142–155. https://doi.org/10.1002/mpr.44
Robins, L. N., Schoenberg, S. P., Holmes, S. J., Ratcliff, K. S., Benham, A., & Works, J. (1985). Early home environment and retrospective recall: A test for concordance between siblings with and without psychiatric disorders. American Journal of Orthopsychiatry, 55(1), 27–41. https://doi.org/10.1111/j.1939-0025.1985.tb03419.x
Ronning, J. A., Sourander, A., Kumpulainen, K., Tamminen, T., Niemela, S., Moilanen, I., Helenius, H., Piha, J., & Almqvist, F. (2009). Cross-informant agreement about bullying and victimization among eight-year-olds: Whose information best predicts psychiatric caseness 10–15 years later? Social Psychiatry and Psychiatric Epidemiology, 44(1), 15–22. https://doi.org/10.1007/s00127-008-0395-0
Schoeler, T., Duncan, L., Cecil, C. M., Ploubidis, G. B., & Pingault, J. B. (2018). Quasi-experimental evidence on short-and long-term consequences of bullying victimization: A meta-analysis. Psychological Bulletin, 144(12), 1229.
Tajima, E. A., Herrenkohl, T. I., Huang, B., & Whitney, S. D. (2004). Measuring child maltreatment: A comparison of prospective parent reports and retrospective adolescent reports. American Journal of Orthopsychiatry, 74(4), 424–435. https://doi.org/10.1037/0002-9432.74.4.424
U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2023). Child maltreatment 2021. https://www.acf.hhs.gov/cb/data-research/child-maltreatment. Accessed 26 Feb 2024
Widom, C. S. (2020). Commentary: A challenge for a higher bar in research on childhood trauma - reflections on Danese (2020). Journal of Child Psychology and Psychiatry, 61(3), 251–254. https://doi.org/10.1111/jcpp.13195
Widom, C. S., Weiler, B. L., & Cottler, L. B. (1999). Childhood victimization and drug abuse: A comparison of prospective and retrospective findings. Journal of Consulting and Clinical Psychology, 67(6), 867–880. https://doi.org/10.1037//0022-006x.67.6.867
Wolke, D., Baumann, N., Strauss, V., Johnson, S., & Marlow, N. (2015). Bullying of preterm children and emotional problems at school age: Cross-culturally invariant effects. The Journal of Pediatrics, 166(6), 1417–1422. https://doi.org/10.1016/j.jpeds.2015.02.055
Wolke, D., & Lereya, S. T. (2015). Long-term effects of bullying. Archives of Disease in Childhood, 100(9), 879–885. https://doi.org/10.1136/archdischild-2014-306667
Wolke, D., & Meyer, R. (1999). Cognitive status, language attainment, and prereading skills of 6-year-old very preterm children and their peers: The Bavarian Longitudinal Study. Developmental Medicine and Child Neurology, 41(2), 94–109. https://doi.org/10.1017/s0012162299000201
Wolke, D., & Sapouna, M. (2008). Big men feeling small: Childhood bullying experience, muscle dysmorphia and other mental health problems in bodybuilders. Psychology of Sport and Exercise, 9(5), 595–604. https://doi.org/10.1016/j.psychsport.2007.10.002
Wolke, D., Woods, S., Bloomfield, L., & Karstadt, L. (2000). The Association between direct and relational bullying and behaviour problems among primary school children. Journal of Child Psychology and Psychiatry, 41(8), 989–1002. https://doi.org/10.1111/1469-7610.00687
Woods, S., & Wolke, D. (2004). Direct and relational bullying among primary school children and academic achievement. Journal of School Psychology, 42(2), 135–155. https://doi.org/10.1016/j.jsp.2003.12.002
Acknowledgements
We would like to thank all current and former Bavarian Longitudinal Study Group members, paediatricians, psychologists and research nurses. We are also extremely grateful to all study participants and their families.
Funding
This study was supported by grants from the German Federal Ministry of Education and Science (BMBF) PKE24, JUG14, 01EP9504 and 01ER0801. DW is supported by UK Research and Innovation (UKRI) under the UK governments Horizon Europe funding guarantee (ERC-AdG award) [grant number EP/X023206/1].
Author information
Authors and Affiliations
Contributions
YN contributed to the conceptualisation of the study, conducted the statistical analysis, and drafted the initial manuscript. NB contributed to the study design and data collection. DW conceptualised and designed the study, obtained funding, and had full access to participant data. All authors contributed to the data interpretation, critically reviewed and revised the manuscript for important intellectual content, approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethical approval
Initial ethical approval was obtained from the Ethics Committee of the University of Munich Children’s Hospital and the Bavarian Health Council. Ethical approval for the follow-up in adulthood was obtained from the Ethical Board of the University Hospital Bonn (reference 159/09).
Informed consent
Parents provided informed written consent within 48 h of their child’s birth and all adult participants provided informed written consent. For adult participants with severe impairment, consent was provided by an assigned guardian.
Conflict of interest
All authors state that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ni, Y., Baumann, N. & Wolke, D. Bullying victimisation in childhood and mental health in early adulthood: comparison of prospective and retrospective reports. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-05788-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-05788-x