
Abstract
Purpose
There remains no standard of care for patients with recurrent and chemorefractory glioblastoma. Re-irradiation (reRT) provides an additional management option. However, published series predominantly focus on small reRT volumes utilizing stereotactic hypofractionated regimens. Concerns regarding toxicity have limited utilisation of reRT for larger recurrences, however this may be mitigated with use of bevacizumab (BEV).
Methods and materials
A prospective database of patients managed with the EORTC-NCIC (Stupp) protocol 60 Gy chemoradiotherapy protocol for glioblastoma between 2007 and 2021 was reviewed for those patients receiving reRT for chemorefractory relapse. Serial MRI and PET were used to establish true progression and exclude patients with pseudoprogression or radionecrosis from reRT. The primary endpoint was overall survival (OS) from date of reRT. Prognostic factors were also assessed.
Results
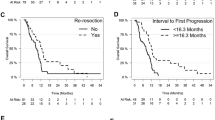
447 patients managed for glioblastoma under the Stupp protocol were identified, of which 372 had relapsed and were thus eligible for reRT. 71 patients underwent reRT. Median relapse-free survival from diagnosis for the reRT and overall cohorts were similar at 11.6 months (95%CI:9.4–14.2) and 11.8 months (95%CI:9.4–14.2) respectively. 60/71 (85%) reRT patients had received BEV prior to reRT and continued concurrent BEV during reRT. Of the 11 patients not managed with BEV during reRT, 10 required subsequent salvage BEV. ReRT patients were younger (median 53 vs. 59 years, p < 0.001), had better performance status (86% vs. 69% ECOG 0–1, p = 0.002) and more commonly had MGMT promoter-methylated tumours (54% vs. 40%, p = 0.083) compared to non-reRT patients. Median reRT PTV volume was 135cm3 (IQR: 69-207cm3). Median OS from reRT to death was 7.1 months (95%CI:6.3–7.9). Patients aged < 50, 50–70 and > 70 years had post-reRT median OS of 7.7, 6.4 and 6.0 months respectively (p = 0.021). Median post-reRT survival was longer for patients with ECOG performance status 0–1 compared to 2–3 (8.1 vs. 6.3 months, p = 0.039). PTV volume, site of relapse, MGMT promoter-methylation status and extent of initial surgical resection were not associated with post-reRT survival. ReRT was well-tolerated. Out of the 6 patients (8%) admitted to hospital after reRT, only one was for reRT toxicity. This was a CTCAE grade 3 radiation necrosis event in a patient managed without prior BEV.
Conclusion
Patients with recurrent glioblastoma who have been previously treated with 60 Gy radiotherapy have a meaningful survival benefit from large volume re-irradiation which is well tolerated. ReRT should not be ignored as a salvage treatment option in patients with chemorefractory progressive disease.

Similar content being viewed by others


References
Minniti G, Niyazi M, Alongi F, Navarria P, Belka C (2021) Current status and recent advances in reirradiation of glioblastoma. Radiation Oncology. 2021;16(1)
Jayamanne D, Wheeler H, Cook R, Teo C, Brazier D, Schembri G et al (2017) Survival improvements with adjuvant therapy in patients with glioblastoma. ANZ J Surg 88(3):196–201. https://doi.org/10.1111/ans.14153
Ghiaseddin A, Peters KB (2015) Use of Bevacizumab in recurrent glioblastoma. CNS Oncol 4(3):157–169. https://doi.org/10.2217/cns.15.8
Levin VA, Bidaut L, Hou P, Kumar AJ, Wefel JS, Bekele BN et al (2011) Randomized double-blind placebo-controlled trial of bevacizumab therapy for radiation necrosis of the central nervous system. IJROBP 79(5):1487–1495. https://doi.org/10.1016/j.ijrobp.2009.12.061
Chan J, Jayamanne D, Wheeler H, Khasraw M, Wong M, Kastelan M et al (2020) The role of large volume re-irradiation with Bevacizumab in chemorefractory high grade glioma. Clin Translational Radiation Oncol 22:33–39
Ho ALK, Jena R (2018) Re-irradiation in the brain: primary gliomas. Clin Oncol 30(2):124–136. https://doi.org/10.1016/j.clon.2017.11.006
Magnuson W, Ian Robins H, Mohindra P, Howard S (2014) Large volume reirradiation as salvage therapy for glioblastoma after progression on bevacizumab. J Neurooncol 117(1):133–139. https://doi.org/10.1007/s11060-014-1363-z
Kim I (2019) Appraisal of re-irradiation for the recurrent glioblastoma in the era of MGMT promotor methylation. Radiat Oncol J 37(1):1–12. https://doi.org/10.3857/Froj.2019.00171
Cuncannon M, Wong M, Jayamanne D, Guo L, Cove N, Wheeler H et al (2019) Role of delayed salvage bevacizumab at symptomatic progression of chemorefractory glioblastoma. BMC Cancer 19(1). https://doi.org/10.1186/s12885-019-5678-1
Tsien CI, Pugh SL, Dicker AP, Raizer JJ, Matuszak MM, Lallana EC et al (2023) NRG Oncology/RTOG1205: a randomized phase II trial of concurrent bevacizumab and reirradiation versus bevacizumab alone as treatment for recurrent glioblastoma. J Clin Oncol 41(6):1285–1295. https://doi.org/10.1200/jco.22.00164
Fokas E, Wacker U, Gross MW, Henzel M, Encheva E, Engenhart-Cabillic R (2009) Hypofractionated stereotactic reirradiation of recurrent glioblastomas. Strahlenther Onkol 185(4):235–240. https://doi.org/10.1007/s00066-009-1753-x
Dixit KS, Sachdev S, Amidei C, Kumthekar P, Kruser TJ, Gondi V et al (2021) A multi-center prospective study of re-irradiation with bevacizumab and temozolomide in patients with bevacizumab refractory recurrent high-grade gliomas. J Neurooncol 155(3):297–306. https://doi.org/10.1007/s11060-021-03875-8
Maranzano E, Anselmo P, Casale M, Trippa F, Carletti S, Principi M et al (2011) Treatment of recurrent glioblastoma with stereotactic radiotherapy: long-term results of a mono-institutional trial. Tumori J 97(1):56–61. https://doi.org/10.1177/030089161109700111
Arpa D, Parisi E, Ghigi G, Savini A, Colangione SP, Tontini L et al (2020) Re-irradiation of recurrent glioblastoma using helical tomotherapy with simultaneous integrated boost: preliminary considerations of treatment efficacy. Sci Rep 10(1). https://doi.org/10.1038/s41598-020-75671-9
Adkison JB, Tomé W, Seo S, Richards GM, Robins HI, Rassmussen K et al (2011) Reirradiation of large-volume recurrent glioma with pulsed reduced-dose-rate radiotherapy. IJROBP 79(3):835–841. https://doi.org/10.1016/j.ijrobp.2009.11.058
Combs SE, Edler L, Rausch R, Welzel T, Wick W, Debus J (2012) Generation and validation of a prognostic score to predict outcome after re-irradiation of recurrent glioma. Acta Oncol 52(1):147–152. https://doi.org/10.3109/0284186x.2012.692882
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the manuscript. E.T. and P.H. authored the main manuscript text, and M.B., H.W., M.W., J.C., and M.K. were instrumental in the conception, design, acquisition and clinical interpretation of the data. V.V. drafted the analysis of the data. All authors reviewed and were involved in the revisions of the manuscript, and M.B. approved the version of the manuscript to be published.
Corresponding author
Ethics declarations
Ethical approval
This study was performed utilising an established prospective patient database approved by the Institutional Ethics Review Board.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tong, E., Horsley, P., Wheeler, H. et al. Hypofractionated re-irradiation with bevacizumab for relapsed chemorefractory glioblastoma after prior high dose radiotherapy: a feasible option for patients with large-volume relapse. J Neurooncol (2024). https://doi.org/10.1007/s11060-024-04643-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11060-024-04643-0