
Abstract
Mental health and, in particular, depression are of great global concern today, especially in middle- and high-income countries. These health issues show an unequal gender prevalence as they are more common in women than in men. The aim of this work is to use micro-econometric models to analyze the prevalence of depression in women in 27 European countries, as well as to quantify the effects of certain individual characteristics on the probability of experiencing depression and the degree to which it occurs. In addition, measures are proposed to assess how each country differs from the total sample. The data used proceed from the European Health Interview Survey wave 2 (EHIS-2). The results show that higher educational levels and incomes are protective factors, while older age and being unemployed have a positive effect on the probability of having depression, particularly on the probability of severe depression. Furthermore, from the calculation of ratios, notable differences are detected in the effects of these characteristics in different countries. Although the direction of the effect of each characteristic is similar in all countries, the size of the effect in each country varies significantly from the sample average. The results highlight the importance of identifying which individual traits generate a higher propensity to experience depression in women. The proposed procedure leads to the conclusion that the detection of differences and similarities between countries could allow the extrapolation of successful practices in prevention and mental health care.
Similar content being viewed by others


The constitution of the World Health Organization defines health as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity (WHO, 2006). This implies that health must be cared for in both its physical and mental aspects. In fact, concern for mental health, understood as psychological and emotional well-being, has grown in recent years, which has generated the need for the design of prevention and promotion plans at all levels.
Moreover, WHO statistics warn about global underinvestment in mental health, emphasizing that most of the targets set for 2020 have not been met. According to Eurostat data, 3.9% of deaths in the EU in 2017 were due to mental and behavioral disorders. Likewise, the latest edition of the Mental Health Atlas notes that although in recent years there has been greater interest and concern for mental health, this has not translated into the expansion or greater quality of care services (WHO, 2021). Indeed, Wahlbeck (2011) emphasizes the weakness of mental health services in Europe and the scarce comparability of data due to differences in contracting services, different diagnostic and recording practices, among others, which make harmonization necessary. In general, two interrelated dimensions of mental health are identified, on the one hand, positive mental health or mental well-being and, on the other, the presence or absence of mental disorders. However, absence of mental disorders is not the only necessary condition for good mental health (Majcherek et al., 2022). The factors that cause one or the other dimension may be different and, in turn, may be considered as different levels of positive mental health (Dreger et al., 2014). Unfortunately, knowledge about mental health disorders, referred to in the literature as mental health literacy and defined as “knowledge and beliefs about mental disorders which aid their recognition, management or prevention” (Jorm, 2000, p. 396), has been neglected compared to the widely accepted knowledge about physical illnesses, both in developing and developed countries (Uddin et al., 2019).
Depression is a prevalent disorder in many countries, exhibiting variations in terms of onset age, recurrence, and its lifelong impact (Kessler & Bromet, 2013). These differences are better understood when considering the cultural and social norms of each country. Musa et al. (2020) highlight significant disparities not only between regions but also in related variables, such as the stigma associated with mental health issues. Notably, the stigma has a more pronounced negative effect in less developed countries, directly impacting economic inequalities. In a similar line, Lim et al. (2018) examines the relationship between certain sociodemographic variables and mental health across different regions. They conclude that countries with lower Human Development Index, particularly those in South America, exhibit a higher prevalence of depression compared to regions like Europe, where the associated risk is lower. Another critical aspect is the therapeutic gap in the effective treatment of mental disorders. Kohn et al. (2004) identifies the global median gap at 56%, representing the difference between the percentage of people requiring and receiving mental health care and those who do not. In this context, Europe stands at 45%, below the global median but showing a higher value compared to specific regions like the Netherlands (21%) that have a more integrated approach to mental health given that they recognize the interconnection between physical and mental health and have implemented its monitoring in primary care, as well as in community settings (Beekman et al., 1997). All the above underscores the importance of conducting studies that consider different regions, as the cultural and social differences inherent to countries can be a significant source of both health and economic inequalities.
Many studies point out that socioeconomic factors, as well as social support, play a fundamental role in health and especially mental health. Fuchs (2004) indicates that health correlates with individual characteristics such as income, educational level, age, and gender. In mental health inequalities, a particularly relevant factor to consider is gender. At the end of the twentieth century, the WHO proposed the first actions linking gender and mental health (WHO, 1998), which materialized in its first gender policy in 2002. In this regard, women have a higher prevalence of certain mental illnesses, such as depression (Basterra, 2017; Valero et al., 2021). Other works that also delve into this idea, that is, the persistent gender inequalities in the risk of depression and the importance of considering the contribution of socioeconomic changes and cultural trends, are those of Kuehner (2016), Smith et al. (2018), and Kiely et al. (2019). This gender difference could be due to biomedical, psychosocial, epidemiological, and even social factors (Afifi, 2007). The same work points out that women are more likely to be diagnosed with depression than men, even when they have the same symptoms or scores on standardized questionnaires. This is an intriguing point to consider. It suggests the possibility that men may be underdiagnosed, and their symptoms might not be recognized as indicative of depression (Faisal-Cury et al., 2022; Shi et al., 2021). Gender inequalities in mental health are also the result of socially established roles and norms, which emphasize the referent role of the male pattern and tend to minimize women’s mental health needs (Valero et al., 2021). The study conducted by Van de Velde et al. (2010), which analyzed the gender gap in depression across 23 European countries, underscores the strong association between socioeconomic factors and depression. They observed that women consistently report higher levels of depression than men across all countries, with significant variations between nations. Similarly, Kessler and Bromet (2013) highlight the connection between sociodemographic traits and severe depression. In a similar line, Seedat et al. (2009) emphasize not only gender differences in prevalence but also the diverse externalization of its effects; specifically, men tend to externalize through increased episodes of violence and substance abuse. All these findings underscore the importance of conducting analyses that contribute to identifying the gender-specific differences in depression, particularly given the distinct and more acute impact this disorder has on women. In this context, for risk factor reduction strategies to be effective, gender must be considered.
The aim of this study is to assess the impact of certain sociodemographic characteristics on the prevalence and degree of depression among women in 27 European countries. To do this, we consider three degrees: the absence (no significant depressive symptoms), the presence of a mild or moderate disorder, and the presence of a severe disorder. The relevance of the analysis lies not only in the quantification in probabilistic terms of the impact of the determinants considered that affect mental health through micro-econometric models but also in the inclusion of a large number of countries in the analysis. The consideration of a broad group of countries implies taking into account the potential differences in cultural, economic, and social terms that these countries present. Specifically, in the case analyzed in this paper, it allows us to observe that, although all the regions are part of the same supranational reality (European Union or European continent), their citizens exhibit notable differences simply because they belong to one country or another. While the various factors considered show a similar effect on the risk of depression, the impact of these effects varies. In summary, the goal is to obtain an overview of the defining characteristics of mental health in the set of countries analyzed and, therefore, to highlight the differences and similarities among them. Thus, this study differs from what is usual in the literature, which only considers one country or a small group (Barone & Barra, 2020; Basterra, 2017; Reile & Sisask, 2021; Uddin et al., 2019, among others).
The paper is structured as follows. The next section describes the data and the methodology used. This is followed by the results, the discussion section, and finally the main conclusions.
Data and Methodology
This study utilizes data from the European Health Interview Survey wave 2 (EHIS-2), conducted by EUROSTAT between 2013 and 2015, representing the most recently accessible data. This survey provides information on the health status of European individuals aged 15 and older, including their physical and mental health status, the presence of chronic diseases, and problems or limitations that have an impact on an individual’s health (Eurostat, 2013).
The initial sample was 171,399 women from 30 countries. Specifically, these countries correspond to the current EU-27, plus Iceland, Norway, and the UK. However, three of them (Belgium, Spain, and the Netherlands) had to be dropped because they did not have the information associated with the mental health module. In addition, some individuals were eliminated due to the absence of valid responses to the variables used. Thus, the final sample used consists of 134,456 women from 27 European countries. Table 1 presents the distribution of the sample of women for each of the sociodemographic characteristics.
Mental health is captured in the EHIS-2 through the PHQ-8 (Patient Heath Questionnaire). This is a validated questionnaire composed of eight items whose aim is to “monitor mental health,” determining the prevalence and degree of severity of a subdimension of mental health problems. Specifically, the questionnaire refers to depressive symptoms and functional impairment and is based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) that establishes criteria for depression. The eight items or questions of the PHQ-8 questionnaire refer to a person’s state in the last 2 weeks on a Likert scale from 0 to 3 (from not at all to almost every day). The sum of the scores on the PHQ-8 ranges from 0 to 24 points. In some studies, a score greater than or equal to 10 points is taken as the cut-off point for classifying individuals. Thus, individuals in the sample for whom the sum of the scores on the scale items meets this criterion are considered to have a depressive disorder (Arias de la Torre et al., 2021; Kroenke et al., 2009; Benatov et al., 2022), and different degrees of severity of depression can be established (Hapke et al., 2019; Kroenke et al., 2001).
In the present study, in order to differentiate the degree of depression that the respondent presents, we chose to consider three categories: a score of 0 to 4 indicates no significant depressive symptoms (from now on, “no mental disorder” or “absence”), 5 to 14 indicates a mild or moderate depressive disorder, and a score above 15 indicates a severe disorder.
Discrete choice models are the methodological tool of this paper. These models are appropriate for contexts in which the variable of interest is discrete in nature, i.e., has a finite number of values or alternatives (Jones, 2007, among others).
The number of alternatives, the ordered or unordered nature of the dependent variable, and the distribution assumed for the vector of disturbance terms will determine the model finally specified. When there are more than two unordered alternatives, a multinomial specification can be chosen. Furthermore, assuming independent type I (Gumbel) extreme value distributions, the multinomial logit model is obtained where the probabilities of each alternative (\(j\)) for an individual (\(i\)) can be expressed:
where \({x}_{i}\) is the vector of explanatory variables and \(\beta\) is the set of parameters to be estimated.
In this study, a multinomial logit model for women in the set of countries is estimated, where the dependent variable, representing degree of depression self-reported, takes the following values: \({Y}_{i}=0\) (absence); \({Y}_{i}=1\) (mild or moderate depression); \({Y}_{i}=2\) (severe depression). Additionally, discrete changes are included, which are calculated from the difference between the probability of each alternative when the individual shows the characteristic in question and when they do not. These changes reflect the effect of each factor with respect to the reference factor in the case of qualitative variables. These discrete changes have been obtained for each of the individuals in the sample, and then, an average has been calculated. The expression for the calculation is
Moreover, a logit binomial model is estimated for women with depression. In this case, where only two alternatives are considered (mild/moderate vs. severe depression), and it represents a particular case of the multinomial model, the probability associated with each of them is obtained by setting J = 1, i.e.,
The probability associated with the reference category (j = 0) is complementary to the previous one.
To approximate a measure that illustrates the distance of the effect of each trait in each country, in relation to the average effect of the set of countries, we propose the calculation of a ratio, expressed as the percentage difference, which quantifies this distance. Obtaining this measure makes it possible to detect notable differences in the effects of the characteristics considered for different countries. Thus, based on the average discrete changes for women in each country, the ratio with respect to the average discrete change has been calculated for all the women in the total sample to analyze in which countries the effect of each trait on the probability presents a greater or lesser difference with respect to the average discrete change. This analysis, in a way, singles out the characteristics through the differences found in the different countries. In addition, to further discuss the results in relation to the countries, it is calculated the frequency distribution of the predicted probabilities in each country to illustrate the behavior of those countries with more differentiated scenarios in terms of the effects on the probabilities calculated for each alternative.
Results
Descriptive Analysis
A descriptive analysis of the data shows that 75.5% of the women have no significant depressive symptoms, 21.7% have mild or moderate depression, and 2.8% have severe depression. In the analysis by country, it is observed that Portugal, Iceland, Luxembourg, Germany, and Hungary have a higher prevalence of depression in the female population, with percentages above 30% (Table 2).
Based on the straightforward analysis of cross-tabulations (found in the supplementary material), we can draw initial conclusions about basic relationships. These findings will be further supported in the analysis of the estimated models. In particular, most of the women in the sample, regardless of whether or not they present a mental disorder, are aged between 30 and 64. Of those who do not have depression, 16% are under 30 years of age and 24.4% are over 65; however, in the majority group of women, it is almost 60%. In relation to educational level, the higher the education level, the lower the percentage of women with a mental psychopathology, although the percentages are higher if compared with the total sample. Results show that 56% of the women with a severe degree of depression have primary education, followed by 30.7% with secondary education and 13.3% with university education. Thus, a negative association was observed between degree of depression and education level.
There is a greater presence of women with lower income levels within the group of those with some degree of depression. In fact, 25.7% and 32.4% of those with a severe disorder have income levels below the second quintile, compared to percentages below 14% for those with higher income levels. As a general trend, the higher the income level, the lower the prevalence of the disease. Of the women with the lowest income level, 4.3% have a severe disorder, compared with 1.3% of those with the highest income level. In addition, 5.9% of the women with moderate depression and 7.5% of those with a severe depression are unemployed (the unemployed category includes actively job-seeking individuals meeting legal employment criteria). Also, 3.8% of unemployed women have a severe disorder compared to 2.7% of those who are in other situation in terms of laboral status and the presence of mild or moderate disorder is also 2 percentage points higher for unemployed women compared to others (see supplementary material).
Econometric Models
To achieve the objectives of this paper, discrete choice models are estimated. First, we present estimates and discrete changes of the specification of a multinomial logit model for women in the set of countries (Table 3) where the dependent variable represents degree of depression: absence, mild or moderate depression, severe depression.
Women under the age of 30 are less prone to experiencing both moderate and severe depression. Thus, the discrete changes associated with the 30–64 and 64 + age ranges confirm that the prevalence of moderate depression is 1.6% and 5.5% higher than for younger women and 0.7% and 1.5% higher for severe depression, respectively.
A higher level of education has a negative impact on the likelihood of having depression, specifically, around 5% less likely to show moderate depression than women with a lower education level. If a woman is unemployed, she is more likely to be depressed (1%) than if she is in other situation. The higher the woman’s income, the lower the probability of presenting depression of any degree. Indeed, it is 8 percentage points lower for women with an income above quintile 5 compared to those with the lowest income.
To further explore the analysis of the association between each individual trait and depressive disorder, discrete changes are calculated for each subsample of women by country. Figure 1 presents the ratio (see “Data and Methodology”) calculated for the three alternatives of the dependent variable in each country and for the characteristics in which greater variability (or dispersion) has been observed. Based on the calculated measure, the relative position of each country is interpreted with respect to the mean and taking into account the sign of the average discrete change for each country. This means that for those countries that are positioned above the value 0, the effect of the analyzed trait has a positive percentage difference with respect to the average discrete change. This is at the value 0 as the ratios are expressed in percentage changes. The main results are highlighted below.

Ratio of differences in the discrete change (multinomial logit model for each degree of depression severity in women)
No Depression Alternative (Graphs 1a–d)
Malta and Portugal stand out with unique sociodemographic patterns. These countries show higher impacts, ranging from 3 to 14% above average, especially for unemployed or 30–64-year-old women in terms of education, age, unemployment, and income. Conversely, Denmark, Estonia, Norway, and Finland exhibit lower impacts compared to the 27-country average. Notably, higher education correlates positively with lower depression risk, but in countries like Norway, below-average percentages suggest that individuals with higher education are less likely to be depression-free. This indicates a less prominent role for the protective effect of educational attainment in these countries. This result should be interpreted considering the national context of the specific country. In essence, it is not merely about the protective role of education for an individual; rather, on average, the level of education may have a more or less significant impact on the prevalence of depression based on the country’s characteristics, compared to the rest of the countries in the group.
Mild/Moderate Depression Alternative (Graphs 1e–h)
The impact of being over 64 on the likelihood of moderate depression varies by country, ranging from 3 below to 5% above the average. Portugal and Malta have the highest ratios, while Denmark, Finland, and Norway have the lowest. Highly educated women in the Czech Republic have an effect 2% higher than the average, with many countries close to the average. For employment status, unemployed women in the Czech Republic or Slovakia are 2% above the average, while those in Malta or Portugal are furthest below. Regarding income levels, Malta and Portugal again show the highest ratio at 4% above the average effect.
Severe Depression Alternative (Graphs 1i–l)
Malta and Portugal stand out for women aged 30–64, with ratios over 30% above the average, while Denmark, Estonia, Norway, and Finland show effects below the average. Tertiary education’s impact varies, with Iceland and Norway below average and the Czech Republic, Malta, and Portugal having the highest ratios (7% above). Unemployment and high income (quintile 5) for women in Malta and Portugal result in effects over 30% above average, contrasting with Estonia or Denmark, nearly 20 percentage points below average. Despite the negative income-depression relationship for all countries, the risk is more pronounced in Portugal, indicating a weaker protective effect of income in this country.
Considering only the subsample of women with depression, a binomial logit model is estimated whose dependent variable takes the following values: Yi = 0 (moderate/mild depression); Yi = 1 (severe depression). The results are shown in Table 4. It can be seen that depressed women over 30 years of age are almost two percentage points more likely to be severely depressed than younger women. As women’s educational level increases, the prevalence of major depression decreases and is lower than for women with primary education. The effect of being unemployed is 2.6% higher and, also, a higher income level increases the probability of moderate rather than severe depression. The effects on the probability of being severely depressed are, in general, more pronounced than those obtained in the multinomial model.
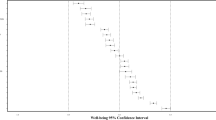
Figure 2 presents the ratios calculated from the ratio of the discrete change for the subsample of women with depression in each country to the average discrete change for women with depression in all countries. The discrete change is found to be above the average at a greater distance for women with depression in Malta and Portugal who are aged 30–64, unemployed, or have the highest income level. The two countries mentioned above have the largest distances from the average effect with percentages close to 20 percentage points above. By contrast, women with depression from Denmark, Estonia, Finland, or Germany have, for the traits indicated, the highest ratios below the average.

Ratio of differences in the discrete change (binomial logit model for severity depression in women)
Figure 3 shows, on the ordinate axis, the proportion of individuals and, on the abscissa axis, on a scale of 1 to 5, intervals of constant amplitude that divide the predicted probability values into five, adjusted to the specific probability range of each region considered. This makes it possible to observe in which probability range most individuals in each country fall. Specifically, four countries are represented, Malta and Portugal which have a close profile according to the effects and, on the other hand, Denmark and Estonia with a different profile. A noteworthy aspect is that a certain similarity in the pattern of behavior is observed in the three alternatives for Malta and Portugal, as opposed to Estonia and Denmark. On the other hand, both for the countries considered and for the whole sample, the proportion of individuals in the intermediate intervals is very close. In particular, in the alternative no depression, the majority of individuals in Denmark and Estonia are in the high probabilities, while in moderate and severe depression these countries have a higher proportion of individuals in the lower probabilities. The opposite is true for Malta and Portugal. This implies that, in Denmark and Estonia, more individuals will be classified as having no depression, since they have a higher average probability. The proposed procedure allows us to conclude that this method is useful for assessing differences and similarities between countries, which, to some extent, could allow the extrapolation of successful practices in prevention and mental health care.

Frequency distribution of predicted probabilities for each degree of depression severity
Discussion
The results obtained indicate that the impact of the sociodemographic traits analyzed on the likelihood of women experiencing a certain level of depression varies based on the country under consideration. Thus, there are certain countries in which the impact is well above the average effect for the countries as a whole, as in the case of Malta and Portugal, while for others, including Northern European countries, the effect is below the average. In this sense, studies such as Wilkinson and Pickett (2006) point out the relationship between health and income inequalities among countries, as well as the role that consideration of different social classes according to each country’s culture can play. In the same line, Bromet et al. (2011) highlight the strong relationship between the social conditions of each country and the prevalence of severe depression in different regions, comparing low- to middle-income countries with high-income countries and finding lower prevalence in the latter, such as Belgium, the Netherlands, France, Italy, and Germany. Knesebeck et al. (2003) and Luppa et al. (2008) delve deeper into this matter for this region. Some studies suggest that nations with greater gender equity are more prone to show larger psychological gender differences, in addition to ethnicity or the need for monitoring for possible changes going forward (Salk et al., 2017). Finally, in line with what has been highlighted in the introduction, the considerable differences in health care systems among European countries may impact proportions of people with symptoms of depression receiving treatment and its adequacy, particularly in the key area of primary care, and require further study (Paykel et al., 2005).
This analysis is of interest insofar as quantifying the differentiated effects for each country can help in the design of an appropriate response in terms of implementing effective policies that consider specific segments of the population. There have been few studies in the literature that have analyzed the prevalence of certain individual traits on women’s mental health, and specifically on depression, that include such a broad set of countries and that quantify differences in effects by country.
The results found in relation to unemployment coincide with those found, for example, in Artazcoz et al. (2004) and Barone and Barra (2020). That is, being unemployed is associated with an increased risk of mental disorder. Artazcoz et al. (2004) point out the possibility of excluding the long-term unemployed from the analysis as their specific reality may provide a more complex context for analysis. The positive effect of income and educational level on a lower risk of depression coincides with that found by Amroussia et al. (2017), Majcherek et al. (2022), and Reile and Sisask (2021), who identify them as protective factors for mental health. However, Basterra (2017) found no evidence of a relationship with educational attainment, although he does establish a clear difference in the prevalence of depression between men and women.
Regarding the effect of age, there is no consensus in the literature. Arias de la Torre et al. (2021) find similar results to the present study and Hapke et al. (2019) also find higher prevalence of depression among older adults in Southern Europe (Italy, Portugal, and Romania). To the contrary, Reile and Sisask (2021) report a higher incidence of different mental health problems among young people compared to those aged 50–64 years old, and Benatov et al. (2022) also find higher ratios for younger people, although they only consider a sample of young adults (20–40 years old).
Despite the potential contributions of this work, it is not without limitations. Existing literature emphasizes the importance of expanding the study of mental health beyond a clinical perspective and adopting a longitudinal approach. The adoption of a longitudinal approach, since the data used are cross-sectional, is not addressed in this work. Analyzing mental health data from this perspective could allow for conclusions to be drawn from a temporal point of view, which could even enable the establishment of causal relationships. On the other hand, the analysis of an individual’s current mental health status is obtained from self-perceived sources, that is, through validated instruments based on self-assessment of different items. This fact implies that the measurement may not be entirely accurate, so it would be advisable to approach it using clinical or diagnosed data. Therefore, extending this work involves incorporating data from different waves of this or other surveys to address this issue from a time perspective.
Conclusions
This paper analyzes the prevalence of depression in the female population of a large number of European countries and determines the impact of characteristics such as unemployment, income, educational level, and age on the prevalence of depression and its severity, based on the estimation of a multinomial logit model for women and a binomial logit model for women with depression. The results obtained make it possible to assess the impact of sociodemographic features that are relevant to mental health and to quantify their effect on the probability of depressive disorder. Moreover, based on the proposal of a measure calculated from ratios between the effects per country and the average effect, it becomes clear that, although the direction of the effect of the different traits is the same for all countries, the size of the effect for the sample of women in each country varies significantly from the average. Precisely, one of the contributions of the paper lies in the quantification of the differences in the impacts of these characteristics in each country.
The analysis is of particular interest because of the prevalence of mental health in women. These differences could be explained by the particularities of the health services and systems in each country, but also by social, cultural, or economic factors in each region. Along these lines, health behaviors, their determinants, and gendered health system responses are three areas where gender influences mental health, as highlighted by the WHO. The consideration of the gender perspective together with the analysis of other socioeconomic determinants, such as those used in this work, reveals the usefulness of this type of study for the proposal of preventive policies.
Across various sociodemographic traits, our analysis reveals distinct patterns influencing mental health outcomes, emphasizing the need for nuanced considerations in mental health research. The interplay between education, age, employment status, and income levels demonstrates the complex relationships shaping the prevalence and severity of depression among women, highlighting the importance of a holistic approach to mental health analysis.
It should be noted that the analysis undertaken illustrates the need to consider policy measures tailored to each country according to the identified traits that generate a higher propensity to experience depression.
References
Afifi, M. (2007). Gender differences in mental health. Singapore Medical Journal, 48(5), 385–391.
Amroussia, N., Gustafsson, P. E., & Mosquera, P. A. (2017). Explaining mental health inequalities in northern Sweden: a decomposition analysis. Global Health Action, 10, 1305814. https://doi.org/10.1080/16549716.2017.1305814
Arias-de la Torre, J., Vilagut, G., Ronaldson, A., Serrano-Blanco, A., Martín, V., Peters, M., Valderas, J. M., Dregan, A., & Alonso, J. (2021). Prevalence and variability of current depressive disorder in 27 European countries: a population-based study. Lancet Public Health, 6, 729–738. https://doi.org/10.1016/s2468-2667(21)00047-5
Artazcoz, L., Benach, J., Borrell, C., & Cortès, I. (2004). Unemployment and mental health: understanding the interactions among gender family roles and social class. American Journal of Public Health, 94(1), 82–88. https://doi.org/10.2105/ajph.94.1.82
Barone, A., & Barra, C. (2020). The relationship between employment and mental health problems in Italy: evidence from EHIS2 microdata. Universitá deli Studi di Salerno, working paper 3.240: 1–31.
Basterra, V. (2017). Evolución de la prevalencia de alto riesgo de trastornos mentales en población adulta española: 2006–2012. Gaceta Sanitaria, 31(4), 324–326. https://doi.org/10.1016/j.gaceta.2017.01.004
Beekman, A., Deeg, D., Braam, A., Smit, J., & Tilburg, W. (1997). Consequences of major and minor depression in later life: a study of disability, well-being and service. Psychological Medicine, 27, 1397–1409.
Benatov, J., Ochnik, D., Rogowska, A. M., Arzensek, A., & Bitenc, U. M. (2022). Prevalence and sociodemographic predictors of mental health in a representative sample of young adults from Germany, Israel, Poland and Slovenia: a longitudinal study during the COVID-19 pandemic. International Journal of Environmental Research and Public Health, 19(1334), 1–18. https://doi.org/10.3390/ijerph190331334
Bromet, E., Andrade, L., Hwang, I., Sampson, N., Alonso, J., de Girolamo, G., de Graaf, R., Demyttenaere, K., Hu, C., Iwata, N., Karam, A., Kaur, J., Kostyuchenki, S., Lépine, J.-P., Levinson, D., Matschinger, H., Medina Mora, M., Browne, M., Posada-Villa, J., … Kessler, R. (2011). Cross-national epidemiology of DSM-IV major depressive episode. BMC Medicine, 9(90), 1–16. https://doi.org/10.1186/1741-7015-9-90
Dreger, S., Buck, C., & Bolte, G. (2014). Material, psychosocial and sociodemographic determinants are associated with positive mental health in Europe: a cross-sectional study. British Medical Journal Open, 4, 1–9. https://doi.org/10.1136/bmjopen-2014-005095
Eurostat. (2013). European Health Interview Survey (EHIS wave 2). Methodological manual. European Commission. https://ec.europa.eu/eurostat/en/web/products-manuals-and-guidelines/-/ks-02-18-240
Faisal-Cury, A., Ziebold, C., de Oliveira, R. D., & Matijasevich, A. (2022). Depression underdiagnosis: prevalence and associated factors. A population-based study. Journal of Psychiatric Research, 151, 157–165. https://doi.org/10.1016/j.jpsychires.2022.04.025
Fuchs, V. R. (2004). Reflections on the socio-economic correlates of health. Journal of Health Economics, 23, 653–661. https://doi.org/10.1016/j.jhealeco.2004.04.004
Hapke, U., Cohrdes, C., & Nübel, J. (2019). Depressive symptoms in a European comparison – results from the European Health Interview Survey (EHIS) 2. Journal of Health Monitoring, 44, 57–65. https://doi.org/10.25646/6227
Jones, A. (2007). Applied econometric for health economists. A practical guide (2nd ed.). Radcliffe Publishing Ltd. https://www.amazon.com/Applied-Econometrics-Health-Economists-Practical/dp/1846191718
Jorm, A. F. (2000). Mental health literacy: public knowledge and beliefs about mental disorders. British Journal of Psychiatry, 177, 396–401. https://doi.org/10.1192/bjp.177.5.396
Kessler, R., & Bromet, E. (2013). The epidemiology of depression across cultures. Annual Review of Public Health, 34, 119–213. https://doi.org/10.1146/Fannurev-publhealth-031912-114409
Kiely, K., Brady, B., & Byles, J. (2019). Gender, mental health and ageing. Maturitas, 129, 76–84. https://doi.org/10.1016/j.maturitas.2019.09.004
Knesebeck, O., Lüschen, G., Cockerham, W., & Siegrist, J. (2003). Socioeconomic status and health among the aged in the United States and Germany: A comparative cross-sectional study. 57, 1643-1652. https://doi.org/10.1016/s0277-9536(03)00020-0
Kohn, R., Saxena, S., Levav, I., & Saraceno, B. (2004). The treatment gap in mental health care. Bulletin of the World Health Organization, 82, 858–866.
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9. Validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Kroenke, K., Striner, T. W., Spitzer, R. L., Williams, J. B. W., Berry, J. T., & Mokdad, A. H. (2009). The PHQ-8 as a measure of current depression in the general population. Journal of Affective Disorders, 114(1–3), 163–1736. https://doi.org/10.1016/j.jad.2008.06.026
Kuehner, C. (2016). Why is depression more common among women than among men? Lancet Psychiatry, 1–13. https://doi.org/10.1016/S2215-0366(16)30263-2
Lim, G., Tam, W., Lu, Y., Ho, C., Zhang, M., & Ho, R. (2018). Prevalence of depression in the community from 30 countries between 1994 and 2014. Scientific Reports, 8(2861), 1–10. https://doi.org/10.1038/s41598-018-21243-x
Luppa, M., Heinrich, S., Matschinger, H., Sandholzer, H., Angermeyer, M., König, H., & Riedel-Heller, S. (2008). Direct costs associated with depression in old age in Germany. 195, 195-204.https://doi.org/10.1016/j.jad.2007.05.008
Majcherek, D., Kowalski, A. M., & Lewandowska, M. S. (2022). Lifestyle, demographic and socio-economic determinants of mental health disorders of employees in the European countries. International Journal of Environmental Research and Public Health, 19(11913), 1–22. https://doi.org/10.3390/ijerph191911913
Musa, A., Ashraf, J., Tsai, F., Abolmagd, S., Liu, C., Hussain, H., Voslarova, E., Khalil, M., Wolitzky-Taylor, K., Lee, D., Sugar, J., Pendi, K., Lee, J., Abdelmaksoud, R., Adel, N., & Baron, D. (2020). Depression severity and depression stigma among students. A survey of universities in five countries. The Journal of Nervous and Mental Disease, 208(11), 884–889. https://doi.org/10.1097/nmd.0000000000001226
Paykel, E., Brugha, T., & Fryers, T. (2005). Size and burden of depressive disorders in Europe. European Neuropsychopharmacology, 15, 411–423. https://doi.org/10.1016/j.euroneuro.2005.04.008
Reile, R., & Sisask, M. (2021). Socio-economic and demographic patterns of mental health complaints among the employed adults in Estonia. PLoS One, 16(10), 1–15. https://doi.org/10.1371/journal.pone.0258827
Salk, R., Hyde, J., & Abramson, L. (2017). Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychological Bulletin, 143(8), 783–822. https://doi.org/10.1037/bul0000102
Seedat, S., Scott, K., Angermeyer, M., …, Kessler, R. (2009). Cross-national associations between gender and mental disorders in the World Health Organization world mental health surveys. Archives of General Psychiatry, 66(7), 785–795. https://doi.org/10.1001/archgenpsychiatry.2009.36
Shi, P., Yang, A., Zhao, Q., Chen, Z., Ren, X., & Dai, Q. (2021). A hypothesis of gender differences in self-reporting symptom of depression: Implications to solve under-diagnosis and under-treatment of depression in males. Frontiers in Psychiatry, 12, 1–10. https://doi.org/10.3389/fpsyt.2021.589687
Smith, D., Mouzon, D., & Elliot, M. (2018). Reviewing the assumptions about men’s mental health: an exploration of the gender binary. American Journal of Men’s Health, 12(1), 78–89. https://doi.org/10.1177/1557988316630953
Uddin, M. N., Bhar, S., & Islam, F. M. A. (2019). An assessment of awareness of mental health conditions and its association with socio-demographic characteristics: a cross-sectional study in a rural district in Bangladesh. BMC Health Services and Research, 19(562), 1–11. https://doi.org/10.1186/s12913-019-4385-6
Valero, E., Martín, U., Bacigalupe, A., & Utzet, M. (2021). The impact of precarious jobs on mental health: a gender-sensitive literature review. International Archive of Occupational and Environmental Health, 94, 577–589. https://doi.org/10.1007/s020420-020-01605-7
Van de Velde, S., Bracke, P., & Levecque, K. (2010). Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Social Science & Medicine, 71, 305–313. https://doi.org/10.1016/j.socscimed.2010.03.035
Wahlbeck, K. (2011). European comparisons between mental health services. Epidemiology and Psychiatric Sciences, 20, 15–18. https://doi.org/10.1017/S2045796011000060
Wilkinson, R., & Pickett, K. (2006). Income inequality and population health: a review and explanation of the evidence. Social Science & Medicine, 62, 1768–1784. https://doi.org/10.1016/j.socscimed.2005.08.036
World Health Organization (1998) Health for all in the twenty-first century. Geneva: World Health Organization; Report no.: A51/5. https://apps.who.int/iris/handle/10665/79743. Accessed 19, December, 2022.
World Health Organization (2006) Constitution of the World Health Organization. https://www.who.int/about/governance/constitution. Accessed 19, December, 2022.
World Health Organization. (2021). Mental health atlas 2020. World Health Organization.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. Work co-financed by the Agencia Canaria de Investigación, Innovación y Sociedad de la Información de la Consejería de Economía, Conocimiento y Empleo y por el Fondo Social Europeo (FSE) Programa Operativo Integrado de Canarias 2014–2020, Eje 3 Tema Prioritario 74 (85%).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
M. Carolina Rodríguez-Donate, Imanol L. Nieto-González, and Ginés Guirao-Peréz declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rodríguez-Donate, M.C., Nieto-González, I.L. & Guirao-Pérez, G. Country Differences in the Effects of Individual Traits on Depression in Women in Europe. Int J Ment Health Addiction (2024). https://doi.org/10.1007/s11469-024-01289-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-024-01289-x