

Age-Related Differences in Vancomycin-Associated Nephrotoxicity and Efficacy in Methicillin-Resistant Staphylococcus aureus Infection: A Comparative Study between Elderly and Adult Patients
 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Patient Enrollment and Characteristics
2.2. Vancomycin Treatment and Clinical Outcomes
2.3. Risk Factor for Nephrotoxicity
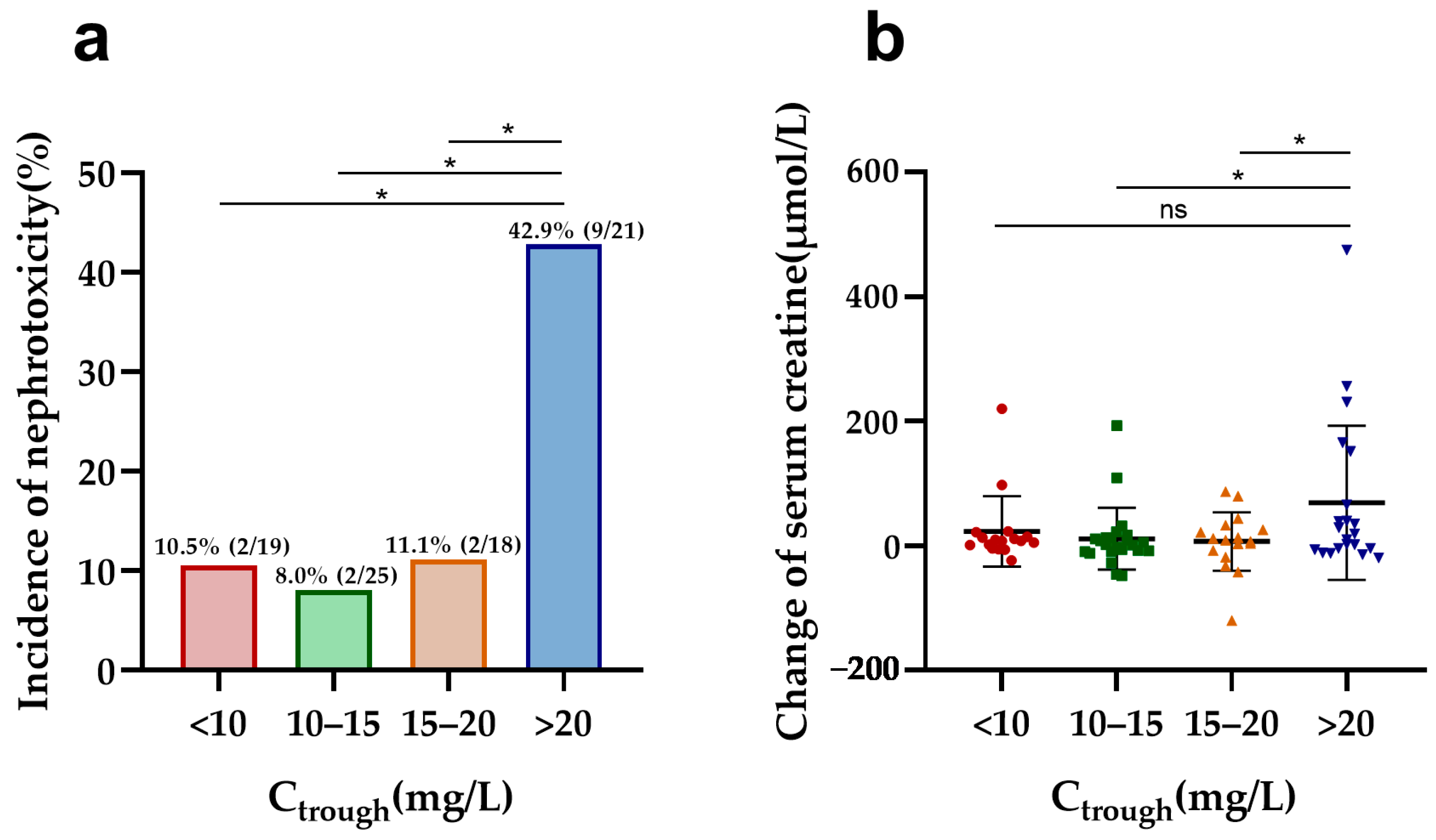
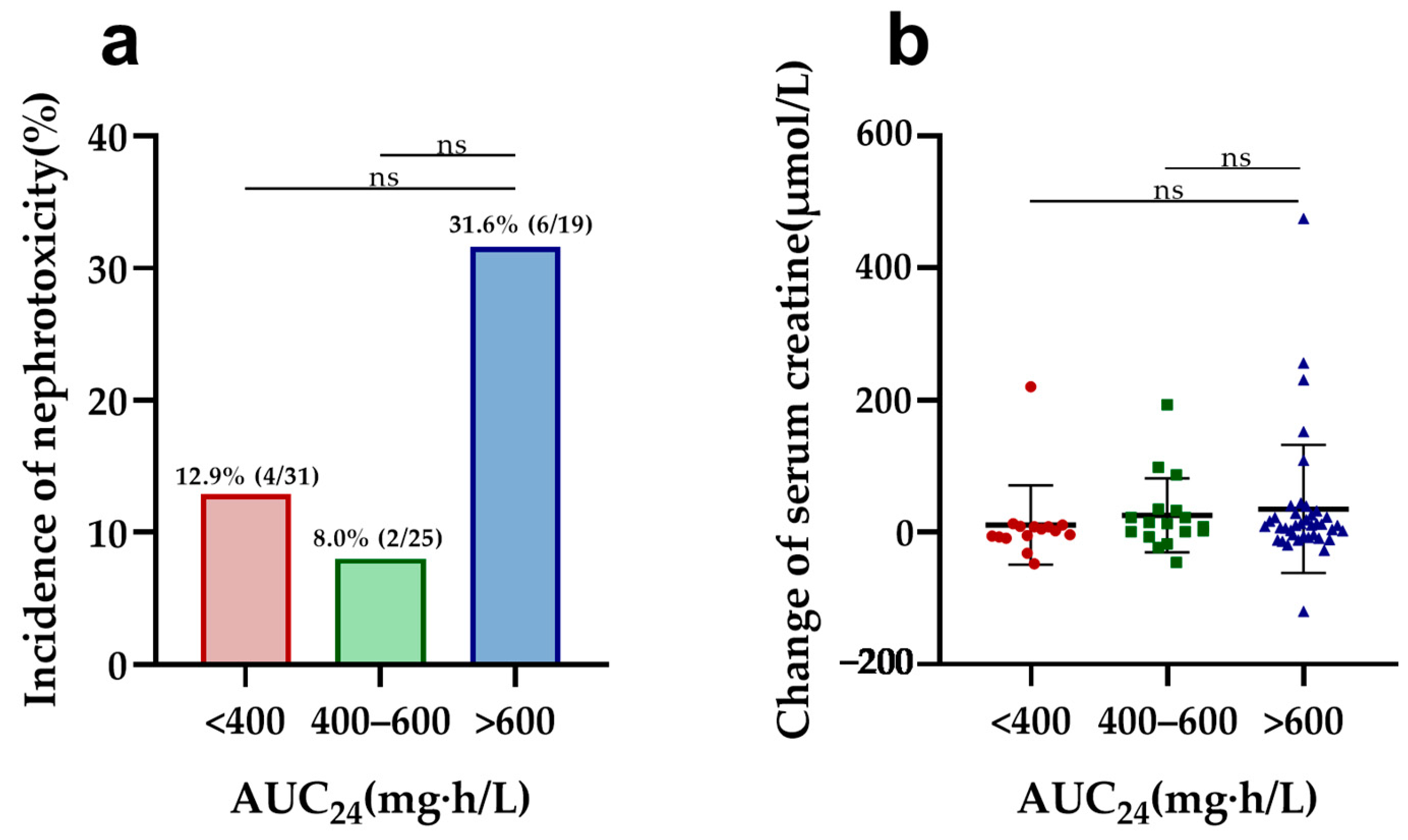
2.4. Associations between Nephrotoxicity and Vancomycin Exposures
2.5. Associations between Nephrotoxicity and Renal Function
3. Discussion
4. Materials and Methods
4.1. Study Design and Data Collection
4.2. Inclusion and Exclusion Criteria
4.3. Microbiological Detection
4.4. Vancomycin TDM and PK/PD Analysis
4.5. Evaluation of Therapeutic Efficacy
4.6. Evaluation of Nephrotoxicity
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin-Loeches, I.; Garduno, A.; Povoa, P.; Nseir, S. Choosing antibiotic therapy for severe community-acquired pneumonia. Curr. Opin. Infect. Dis. 2022, 35, 133–139. [Google Scholar] [CrossRef]
- Tacconelli, E.; Pop-Vicas, A.E.; D’Agata, E.M. Increased mortality among elderly patients with meticillin-resistant Staphylococcus aureus bacteraemia. J. Hosp. Infect. 2006, 64, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Fukumori, S.; Tsuji, Y.; Mizoguchi, A.; Kasai, H.; Ishibashi, T.; Iwamura, N.; To, H. Association of the clinical efficacy of vancomycin with the novel pharmacokinetic parameter area under the trough level (AUTL) in elderly patients with hospital-acquired pneumonia. J. Clin. Pharm. Ther. 2016, 41, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American society of health-system pharmacists, the infectious diseases society of America, the pediatric infectious diseases society, and the society of infectious diseases pharmacists. Clin. Infect. Dis. 2020, 71, 1361–1364. [Google Scholar] [PubMed]
- He, N.; Su, S.; Ye, Z.; Du, G.; He, B.; Li, D.; Liu, Y.; Yang, K.; Zhang, X.; Zhang, Y.; et al. Evidence-based guideline for therapeutic drug monitoring of vancomycin: 2020 update by the division of therapeutic drug monitoring, Chinese pharmacological society. Clin. Infect. Dis. 2020, 71 (Suppl. S4), S363–S371. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Abbas, M.; Nassar, L.; Ghrayeb, A.; Shepshelovich, D.; Kurnik, D.; Leibovici, L.; Paul, M. Attention to age: Similar dosing regimens lead to different vancomycin levels among older and younger patients. Age Ageing 2019, 49, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Lodise, T.P.; Drusano, G. Vancomycin area under the curve-guided dosing and monitoring for adult and pediatric patients with suspected or documented serious methicillin-resistant Staphylococcus aureus infections: Putting the safety of our patients first. Clin. Infect. Dis. 2021, 72, 1497–1501. [Google Scholar] [CrossRef] [PubMed]
- Aljefri, D.M.; Avedissian, S.N.; Rhodes, N.J.; Postelnick, M.J.; Nguyen, K.; Scheetz, M.H. Vancomycin area under the curve and acute kidney injury: A meta-analysis. Clin. Infect. Dis. 2019, 69, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- Holmes, N.E.; Turnidge, J.D.; Munckhof, W.J.; Robinson, J.O.; Korman, T.M.; O’Sullivan, M.V.; Anderson, T.L.; Roberts, S.A.; Warren, S.J.; Gao, W.; et al. Vancomycin AUC/MIC ratio and 30-day mortality in patients with Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 2013, 57, 1654–1663. [Google Scholar] [CrossRef]
- Barber, K.E.; Bell, A.M.; Stover, K.R.; Wagner, J.L. Intravenous vancomycin dosing in the elderly: A focus on clinical issues and practical application. Drugs Aging 2016, 33, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Guay, D.R.; Vance-Bryan, K.; Gilliland, S.; Rodvold, K.; Rotschafer, J. Comparison of vancomycin pharmacokinetics in hospitalized elderly and young patients using a Bayesian forecaster. J. Clin. Pharmacol. 1993, 33, 918–922. [Google Scholar] [CrossRef]
- Fujii, T.; Uchino, S.; Takinami, M.; Bellomo, R. Validation of the kidney disease improving global outcomes criteria for AKI and comparison of three criteria in hospitalized patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Jiang, L.; Du, B.; Wen, Y.; Wang, M.; Xi, X. A comparison of different diagnostic criteria of acute kidney injury in critically ill patients. Crit. Care 2014, 18, R144. [Google Scholar] [CrossRef]
- Jeffres, M.N. The Whole price of vancomycin: Toxicities, troughs, and time. Drugs 2017, 77, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dai, N.; Wei, W.; Jiang, C. Outcomes and nephrotoxicity associated with vancomycin treatment in patients 80 years and older. Clin. Interv. Aging 2021, 16, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Dai, N.; Jiang, C.; Wang, Y. Relationship between vancomycin-induced nephrotoxicity and vancomycin trough concentration in older adults: A retrospective observational study. Indian. J. Pharmacol. 2023, 55, 155–161. [Google Scholar] [PubMed]
- Patel, N.; Pai, M.P.; Rodvold, K.A.; Lomaestro, B.; Drusano, G.L.; Lodise, T.P. Vancomycin: We can’t get there from here. Clin. Infect. Dis. 2011, 52, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Drennan, P.G.; Begg, E.J.; Gardiner, S.J.; Kirkpatrick, C.M.J.; Chambers, S.T. The dosing and monitoring of vancomycin: What is the best way forward? Int. J. Antimicrob. Agents 2019, 53, 401–407. [Google Scholar] [CrossRef]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and functional changes with the aging kidney. Adv. Chronic Kidney Dis. 2016, 23, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.W.; Ji, S.M.; He, X.R.; Zhu, X.; Chen, R.; Lu, W. Influences of renal function descriptors on population pharmacokinetic modeling of vancomycin in Chinese adult patients. Acta Pharmacol. Sin. 2018, 39, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Cutler, N.R.; Narang, P.K.; Lesko, L.J.; Ninos, M.; Power, M. Vancomycin disposition: The importance of age. Clin. Pharmacol. Ther. 1984, 36, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Lim, N.R.; Park, H.J.; Yang, J.W.; Kim, M.J.; Kim, K.; In, Y.W.; Lee, Y.M. Evaluation of risk factors for vancomycin-induced nephrotoxicity. Int. J. Clin. Pharm. 2018, 40, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, T.; Miljkovic, B.; Kovacevic, P.; Dragic, S.; Momcicevic, D.; Avram, S.; Jovanovic, M.; Vucicevic, K. Population pharmacokinetic model of vancomycin based on therapeutic drug monitoring data in critically ill septic patients. J. Crit. Care 2020, 55, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Nowack, M.C.; Hapfelmeier, A.; Umgelter, A.; Schultheiss, C.; Thies, P.; Phillip, V.; Eyer, F.; Schmid, R.M.; Huber, W. Continuous intravenous administration of vancomycin in medical intensive care unit patients. J. Crit. Care 2013, 28, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Vu, D.H.; Nguyen, D.A.; Delattre, I.K.; Ho, T.T.; Do, H.G.; Pham, H.N.; Dao, X.C.; Tran, N.T.; Nguyen, G.B.; Van Bambeke, F.; et al. Determination of optimal loading and maintenance doses for continuous infusion of vancomycin in critically ill patients: Population pharmacokinetic modelling and simulations for improved dosing schemes. Int. J. Antimicrob. Agents 2019, 54, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Filippone, E.J.; Kraft, W.K.; Farber, J.L. The nephrotoxicity of vancomycin. Clin. Pharmacol. Ther. 2017, 102, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Liao, C.H.; Wang, J.L.; Chiang, W.C.; Lai, M.S.; Chie, W.C.; Chang, S.C.; Hsueh, P.R. Method-specific performance of vancomycin MIC susceptibility tests in predicting mortality of patients with methicillin-resistant Staphylococcus aureus bacteraemia. J. Antimicrob. Chemother. 2014, 69, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing; CLSI: Wayne, PA, USA, 2023. [Google Scholar]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: Executive summary. Clin. Infect. Dis. 2011, 52, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.X.; Chen, M.T.; Li, N.Y.; Liu, X.F.; Yang, M.J.; Chen, Y.C.; Liang, X.Y.; Wu, J.F.; Guo, B.N.; Song, S.C.; et al. Sequence Type 5 (ST5) as a Possible Predictor of Bacterial Persistence in Adult Patients with Methicillin-Resistant Staphylococcus aureus Pneumonia Treated with Vancomycin. Microbiol. Spectr. 2022, 10, e0134822. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.; Shoyinka, A.; Chen, A.; Jacobsen, G.; Zervos, M. Evaluation of vancomycin serum trough concentrations and out comes in meticillin-resistant Staphylococcus aureus bacteraemia. Int. J. Antimicrob. Agents 2012, 40, 474–475. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (n = 164) | Elderly Patients (n = 83) | Adult Patients (n = 81) | p Value |
|---|---|---|---|---|
| Demographics | ||||
| Sex | ||||
| Male | 114 (69.5) | 53 (63.9) | 61 (75.3) | 0.111 |
| Female | 50 (30.5) | 30 (36.1) | 20 (24.7) | |
| Age (y) | 66 (53, 80) | 80 (75, 85) | 53 (40, 60) | <0.001 |
| BMI (kg/m2) | 22.16 (19.97, 24.00) | 22.00 (19.53, 24.00) | 22.60 (20.01, 24.22) | 0.324 |
| Renal function | ||||
| Initial serum creatinine (µmol/L) | 59.00 (46.00, 76.00) | 64.00 (48.00, 95.50) | 58.00 (44.50, 70.00) | 0.181 |
| Initial eGFR (mL/min/1.73 m2) | 112.08 (85.41, 146.63) | 102.01 (62.32, 140.23) | 125.04 (97.66, 162.12) | 0.002 |
| Final serum creatinine (µmol/L) | 56.00 (41.75, 80.25) | 64.50 (44.75, 98.25) | 51.00 (39.00, 65.00) | 0.002 |
| Final eGFR (mL/min/1.73 m2) | 122.00 (80.07, 168.77) | 94.27 (60.17, 127.88) | 142.30 (111.21, 191.42) | <0.001 |
| Change in serum creatinine (µmol/L) | 2.00 (−7.50, 14.35) | 8.00 (−6.00, 26.75) | −2.00 (−9.00, 7.00) | 0.004 |
| Comorbidities | ||||
| Cardiovascular disease | 56 (34.1) | 43 (51.8) | 13 (16.0) | <0.001 |
| Diabetes mellitus | 27 (16.5) | 22 (26.5) | 5 (6.2) | <0.001 |
| Stroke | 53 (32.3) | 36 (43.4) | 17 (21.0) | 0.002 |
| COPD | 9 (5.5) | 9 (10.8) | 0 (0.0) | 0.003 |
| Autoimmune disease | 5 (3.0) | 2 (2.4) | 3 (3.7) | 0.680 |
| Trauma | 17 (10.4) | 7 (8.4) | 10 (12.3) | 0.411 |
| Malignancy | 30 (18.4) | 13 (15.7) | 17 (21.3) | 0.357 |
| Hematological malignancy | 1 (0.6) | 1 (1.2) | 0 (0.0) | >0.999 |
| Other diseases | 37 (22.6) | 20 (24.1) | 17 (21.0) | 0.634 |
| Exposures | ||||
| Surgery | 76 (46.3) | 22 (26.5) | 54 (66.7) | <0.001 |
| Vascular catheter | 110 (67.1) | 53 (63.9) | 57 (70.4) | 0.375 |
| Urinary catheter | 94 (57.3) | 45 (54.2) | 49 (60.5) | 0.416 |
| Tracheal cannula | 50 (30.5) | 24 (28.9) | 26 (32.1) | 0.658 |
| Tracheotomy | 42 (25.6) | 13 (15.7) | 29 (35.8) | 0.003 |
| Drainage tube | 41 (25.0) | 14 (16.9) | 27 (33.3) | 0.015 |
| ICU admission | 92 (56.1) | 45 (54.2) | 47 (58.0) | 0.623 |
| ICU duration | 26.50 (17.25, 40.00) | 28.00 (18.50, 47.50) | 26.00 (15.00, 35.00) | 0.246 |
| Infection site | ||||
| Bloodstream infection | 20 (12.2) | 8 (9.6) | 12 (14.8) | 0.311 |
| Pneumonia | 113 (68.9) | 64 (77.1) | 49 (60.5) | 0.022 |
| CNSI | 4 (2.4) | 1 (1.2) | 3 (3.7) | 0.364 |
| SSTI | 18 (11.0) | 3 (3.6) | 15 (18.5) | 0.002 |
| UTI | 7 (4.3) | 6 (7.2) | 1 (1.2) | 0.117 |
| Other infection | 14 (8.5) | 5 (6.0) | 9 (11.1) | 0.244 |
| Concomitant antibiotics | ||||
| β-lactams | 93 (56.7) | 45 (54.2) | 48 (59.3) | 0.515 |
| Rifampicin | 12 (7.3) | 7 (8.4) | 5 (6.2) | 0.578 |
| Quinolones | 6 (3.7) | 0 (0.0) | 6 (7.4) | 0.013 |
| Others | 39 (23.8) | 19 (22.9) | 20 (24.7) | 0.787 |
| Vancomycin use parameters | ||||
| Daily dose (g) | 1.9 (1.2, 2.0) | 1.4 (1.0, 2.0) | 2.0 (1.8, 2.2) | <0.001 |
| Duration (d) | 12 (9, 17) | 12 (9, 16) | 13 (10, 18) | 0.448 |
| Ctrough (mg/L) | 10.88 (6.43, 15.92) | 14.69 (10.58, 20.71) | 7.82 (4.52, 12.57) | <0.001 |
| Cpeak (mg/L) a | 25.66 (19.59, 31.84) | 26.63 (20.15, 32.94) | 24.49 (19.04, 24.49) | 0.112 |
| AUC24 (mg·h/L) b | 404.19 (319.44, 547.20) | 461.65 (353.01, 609.10) | 387.56 (283.53, 462.09) | 0.006 |
| Vancomycin MIC ≥ 1 mg/L c | 90 (55.2) | 41 (50.0) | 49 (60.5) | 0.178 |
| AUC24/MIC b | 562.73 (363.38, 794.90) | 647.97 (461.65, 913.42) | 463.54 (330.09, 718.28) | 0.007 |
| Outcome | ||||
| Clinical success | 112 (68.3) | 56 (67.5) | 56 (69.1) | 0.819 |
| Microbiological success | 127 (77.4) | 64 (77.1) | 63 (77.8) | 0.918 |
| Nephrotoxicity | 20 (12.2) | 15 (18.1) | 5 (6.2) | 0.020 |
| Variables | Elderly Patients (n = 83) | Adult Patients (n = 81) | ||||
|---|---|---|---|---|---|---|
| Non-Nephrotoxicity (n = 68) | Nephrotoxicity (n = 15) | p Value | Non-Nephrotoxicity (n = 76) | Nephrotoxicity (n = 5) | p Value | |
| Demographics | ||||||
| Sex | ||||||
| Male | 44 (64.7) | 9 (60.0) | 0.731 | 58 (76.3) | 3 (60.0) | 0.593 |
| Female | 24 (35.3) | 6 (40.0) | 18 (23.7) | 2 (40.0) | ||
| Age (y) | 80 (74, 86) | 79 (75, 84) | 0.817 | 53 (39, 59) | 46 (35, 63) | 0.898 |
| BMI (kg/m2) | 21.48 (19.53, 23.83) | 22.93 (19.67, 24.08) | 0.516 | 22.16 (20.00, 24.22) | 18.25 (8.32, 27.66) | 0.331 |
| Renal function | ||||||
| Initial serum creatinine (µmol/L) | 61.00 (44.00, 91.75) | 70.60 (52.00, 106.00) | 0.161 | 57.00 (43.00, 59.00) | 121.00 (72.00, 353.50) | 0.011 |
| Initial eGFR (mL/min/1.73 m2) | 104.48 (62.81, 143.68) | 94.59 (45.70, 112.08) | 0.113 | 127.72 (102.16, 172.91) | 52.37 (22.38, 93.40) | 0.003 |
| Final serum creatinine (µmol/L) | 56.80 (42.00, 79.00) | 169.00 (102.00, 255.00) | <0.001 | 50.00 (39.00, 60.00) | 259.40 (93.00, 425.50) | 0.052 |
| Final eGFR (mL/min/1.73 m2) | 108.27 (81.74, 148.24) | 34.77 (18.43, 60.65) | <0.001 | 145.41 (118.18, 194.04) | 23.66 (11.98, 64.98) | <0.001 |
| Change in serum creatinine (µmol/L) | 2.80 (−8.00, 13.00) | 98.00 (40.00, 220.00) | <0.001 | −3.00 (−9.25, 5.25) | 153.80 (18.50, 405.00) | <0.001 |
| Exposures | ||||||
| Surgery | 14 (20.6) | 8 (53.3) | 0.020 | 52 (68.4) | 2 (40.0) | 0.327 |
| Vascular catheter | 42 (61.8) | 11 (73.3) | 0.399 | 54 (74.1) | 3 (60.0) | 0.630 |
| Urinary catheter | 35 (51.5) | 10 (66.7) | 0.285 | 47 (61.8) | 2 (40.0) | 0.379 |
| Tracheal cannula | 19 (27.9) | 5 (33.3) | 0.756 | 24 (31.6) | 2 (40.0) | 0.654 |
| Tracheotomy | 11 (16.2) | 2 (13.3) | >0.999 | 27 (35.5) | 2 (40.0) | >0.999 |
| Drainage tube | 8 (11.8) | 6 (40.0) | 0.017 | 25 (32.9) | 2 (40.0) | >0.999 |
| ICU admission | 33 (48.5) | 12 (80.0) | 0.027 | 43 (56.6) | 4 (80.0) | 0.392 |
| ICU duration | 28.00 (18.25, 47.75) | 27.00 (10.00, 43.00) | 0.075 | 26.00 (12.00, 35.75) | 24.00 (21.00, 25.50) | 0.668 |
| Infection site | ||||||
| Bloodstream infection | 5 (7.4) | 3 (20.0) | 0.153 | 11 (14.5) | 1 (20.0) | 0.561 |
| Pneumonia | 53 (77.9) | 11 (73.3) | 0.738 | 45 (59.2) | 4 (80.0) | 0.643 |
| CNSI | 1 (1.5) | 0 (0.0) | >0.999 | 3 (3.9) | 0 (0.0) | >0.999 |
| SSTI | 2 (2.9) | 1 (6.7) | 0.455 | 15 (19.7) | 0 (0.0) | 0.578 |
| UTI | 5 (7.4) | 1 (6.7) | >0.999 | 1 (1.3) | 0 (0.0) | >0.999 |
| Other infection | 5 (7.4) | 0 (0.0) | 0.579 | 9 (11.8) | 0 (0.0) | >0.999 |
| Concomitant antibiotics | ||||||
| β-lactam | 35 (51.5) | 10 (66.7) | 0.285 | 43 (56.6) | 5 (100.0) | 0.076 |
| Rifampicin | 5 (7.4) | 2 (13.3) | 0.605 | 5 (6.6) | 0 (0.0) | >0.999 |
| Other | 15 (22.1) | 4 (26.7) | 0.738 | 18 (23.7) | 2 (40.0) | 0.593 |
| Vancomycin use parameters | ||||||
| Daily dose (g) | 1.39 (1.00, 2.00) | 1.50 (0.80, 2.00) | 0.806 | 2.00 (1.90–2.20) | 1.25 (0.66, 2.10) | 0.068 |
| Duration (d) | 13.00 (10.00, 16.00) | 10.00 (8.00, 13.00) | 0.133 | 13.00 (10.00, 18.75) | 10.00 (6.50, 10.00) | 0.019 |
| Cpeak (mg/L) a | 25.96 (19.13, 31.95) | 33.62 (26.40, 42.26) | 0.012 | 24.01 (18.63, 29.78) | 39.91 (27.67, 58.01) | 0.009 |
| Ctrough (mg/L) | 13.94 (9.96, 17.69) | 22.65 (14.60, 26.13) | 0.004 | 7.57 (4.41, 11.07) | 25.93 (10.63, 43.45) | 0.004 |
| <10 | 17 (25.0) | 2 (13.3) | 0.502 | 55 (72.4) | 1 (20.0) | 0.030 |
| 10–15 | 23 (33.8) | 2 (13.3) | 0.212 | 13 (17.1) | 1 (20.0) | >0.999 |
| 15–20 | 16 (23.5) | 2 (13.3) | 0.505 | 7 (9.2) | 0 (0.0) | >0.999 |
| >20 | 12 (17.6) | 9 (60.0) | 0.002 | 1 (1.3) | 3 (60.0) | <0.001 |
| AUC24 (mg·h/L) b | 450.01 (353.01, 561.77) | 600.06 (340.53, 725.64) | 0.060 | 367.32 (281.66, 456.82) | 762.40 (664.80, 1022.70) | <0.001 |
| <400 | 27 (42.9) | 4 (33.3) | 0.751 | 45 (60.8) | 0 (0.0) | 0.012 |
| 400–600 | 23 (36.5) | 2 (16.7) | 0.316 | 24 (32.4) | 0 (0.0) | 0.316 |
| >600 | 13 (20.6) | 6 (50.0) | 0.064 | 5 (6.8) | 5 (100.0) | <0.001 |
| Vancomycin MIC ≥ 1 mg/L c | 33 (49.3) | 8 (53.3) | 0.775 | 48 (63.2) | 1 (20.0) | 0.077 |
| AUC24/MIC b | 647.97 (442.72, 928.38) | 681.81 (583.16, 859.99) | 0.298 | 459.44 (328.73, 673.82) | 1524.80 (1019.00, 2045.40) | 0.001 |
| <400 | 14 (22.2) | 1 (8.3) | 0.439 | 30 (40.5) | 0 (0.0) | 0.151 |
| 400–600 | 16 (25.4) | 4 (33.3) | 0.723 | 22 (29.7) | 0 (0.0) | 0.315 |
| >600 | 33 (52.4) | 7 (58.3) | 0.705 | 22 (29.7) | 5 (100.0) | 0.004 |
| Characteristics | Univariate Analysis | Multivariate Logistic Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | aOR (95% CI) | p Value | |
| Surgery | 4.408 (1.365–14.237) | 0.013 | 3.933 (0.821–18.839) | 0.087 |
| Drainage tube | 5.000 (1.405–17.793) | 0.013 | 1.838 (0.185–18.218) | 0.603 |
| ICU admission | 4.242 (1.098–16.391) | 0.036 | 4.177 (0.695–25.089) | 0.118 |
| Cpeak (mg/L) | 1.035 (0.997–1.075) | 0.072 | 1.003 (0.944–1.066) | 0.913 |
| Ctrough (mg/L) | 1.132 (1.044–1.228) | 0.003 | ||
| Reference, <10 | 0.462 (0.094–2.256) | 0.340 | - | - |
| 10–15 (exclude 15) | 0.301 (0.063–1.449) | 0.134 | 0.520 (0.052–5.153) | 0.576 |
| 15–20 | 0.500 (0.102–2.453) | 0.393 | 0.510 (0.047–5.491) | 0.579 |
| >20 | 7.000 (2.095–23.394) | 0.002 | 8.936 (1.943–41.095) | 0.005 |
| AUC24 (mg·h/L) | 1.003 (1.000–1.006) | 0.049 | ||
| Reference, <400 | 0.667 (0.182–2.446) | 0.541 | - | - |
| 400–600 | 0.348 (0.070–1.727) | 0.196 | 0.374 (0.049–2.873) | 0.344 |
| >600 | 3.500 (0.975–12.563) | 0.055 | 0.583 (0.028–11.958) | 0.726 |
| Variables | Elderly Patients (n = 65) | Adult Patients (n = 75) | p Value |
|---|---|---|---|
| Demographics | |||
| Sex | |||
| Male | 42 (64.6) | 56 (74.7) | 0.196 |
| Female | 23 (35.4) | 19 (25.3) | |
| Age (y) | 80 (74, 86) | 53 (39, 59) | <0.001 |
| BMI (kg/m2) | 21.97 (19.54, 23.44) | 22.09 (20.00, 24.21) | 0.373 |
| Renal function | |||
| Initial serum creatinine (µmol/L) | 53.00 (40.50, 68.00) | 56.00 (43.00, 69.00) | 0.756 |
| Initial eGFR (mL/min/1.73 m2) | 111.67 (95.34, 150.13) | 127.72 (103.64, 172.91) | 0.076 |
| Final serum creatinine (µmol/L) | 56.80 (42.00, 79.50) | 50.00 (39.00, 62.25) | 0.016 |
| Final eGFR (mL/min/1.73 m2) | 108.72 (81.79, 150.33) | 144.80 (117.86, 195.22) | <0.001 |
| Change in serum creatinine (µmol/L) | 9.00 (−3.00, 22.65) | −2.50 (−9.00, 6.25) | <0.001 |
| Exposures | |||
| Surgery | 16 (24.6) | 51 (68.0) | <0.001 |
| Vascular catheter | 41 (63.1) | 54 (72.0) | 0.260 |
| Urinary catheter | 37 (56.9) | 46 (61.3) | 0.596 |
| Tracheal cannula | 18 (27.7) | 24 (32.0) | 0.579 |
| Tracheotomy | 10 (15.4) | 28 (37.3) | 0.004 |
| Drainage tube | 10 (15.4) | 26 (34.7) | 0.009 |
| ICU admission | 33 (50.8) | 32 (42.7) | 0.397 |
| ICU duration | |||
| Infection site | |||
| Bloodstream infection | 7 (10.8) | 11 (14.7) | 0.492 |
| Pneumonia | 49 (75.4) | 44 (58.7) | 0.037 |
| CNSI | 1 (1.5) | 3 (4.0) | 0.623 |
| SSTI | 3 (4.6) | 15 (20.0) | 0.007 |
| UTI | 5 (7.7) | 1 (1.3) | 0.096 |
| Other infection | 4 (6.2) | 9 (12.0) | 0.235 |
| Concomitant antibiotics | |||
| β-lactam | 35 (53.8) | 42 (56.0) | 0.798 |
| Rifampicin | 6 (9.2) | 5 (6.7) | 0.574 |
| Quinolones | 0 (0.0) | 5 (6.7) | 0.034 |
| Other | 15 (23.1) | 18 (24.0) | 0.898 |
| Vancomycin use parameters | |||
| Daily dose (g) | 1.50 (1.00, 2.00) | 2.0 (1.91, 2.20) | <0.001 |
| Duration (d) | 12 (10, 16.5) | 13 (10, 18) | 0.518 |
| Ctrough (mg/L) | 13.87 (9.83, 20.16) | 7.50 (4.38, 11.36) | <0.001 |
| Cpeak (mg/L) a | 26.38 (19.43, 32.89) | 24.12 (18.46, 29.43) | 0.112 |
| AUC24 (mg·h/L) b | 450.01 (353.01, 587.96) | 359.14 (281.49, 457.33) | 0.004 |
| Vancomycin MIC ≥ 1 mg/L c | 30 (46.9) | 48 (64.0) | 0.043 |
| AUC24/MIC b | 653.88 (467.90, 900.02) | 458.33 (328.12, 668.66) | 0.001 |
| Outcome | |||
| Clinical success | 45 (69.2) | 51 (68.0) | 0.876 |
| Microbiological success | 50 (76.9) | 58 (77.3) | 0.954 |
| Total success | 43 (66.2) | 49 (65.3) | 0.919 |
| Nephrotoxicity | 10 (15.4) | 2 (2.7) | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xi, L.; Li, S.; Chen, M.; Huang, X.; Li, N.; Chen, N.; Wu, H.; Bian, Q.; Bian, X.; Li, X.; et al. Age-Related Differences in Vancomycin-Associated Nephrotoxicity and Efficacy in Methicillin-Resistant Staphylococcus aureus Infection: A Comparative Study between Elderly and Adult Patients. Antibiotics 2024, 13, 324. https://doi.org/10.3390/antibiotics13040324
Xi L, Li S, Chen M, Huang X, Li N, Chen N, Wu H, Bian Q, Bian X, Li X, et al. Age-Related Differences in Vancomycin-Associated Nephrotoxicity and Efficacy in Methicillin-Resistant Staphylococcus aureus Infection: A Comparative Study between Elderly and Adult Patients. Antibiotics. 2024; 13(4):324. https://doi.org/10.3390/antibiotics13040324
Chicago/Turabian StyleXi, Lin, Shanshan Li, Mengting Chen, Xiaolan Huang, Nanyang Li, Nanye Chen, Hailan Wu, Qiyu Bian, Xingchen Bian, Xin Li, and et al. 2024. "Age-Related Differences in Vancomycin-Associated Nephrotoxicity and Efficacy in Methicillin-Resistant Staphylococcus aureus Infection: A Comparative Study between Elderly and Adult Patients" Antibiotics 13, no. 4: 324. https://doi.org/10.3390/antibiotics13040324