
Negative Pressure Wound Therapy—A Vacuum-Mediated Positive Pressure Wound Therapy and a Closer Look at the Role of the Laser Doppler
 , and
, and
Abstract
:1. Background
2. Methods
3. Participants
4. Study Protocol
4.1. In Vivo Perfusion Measurement
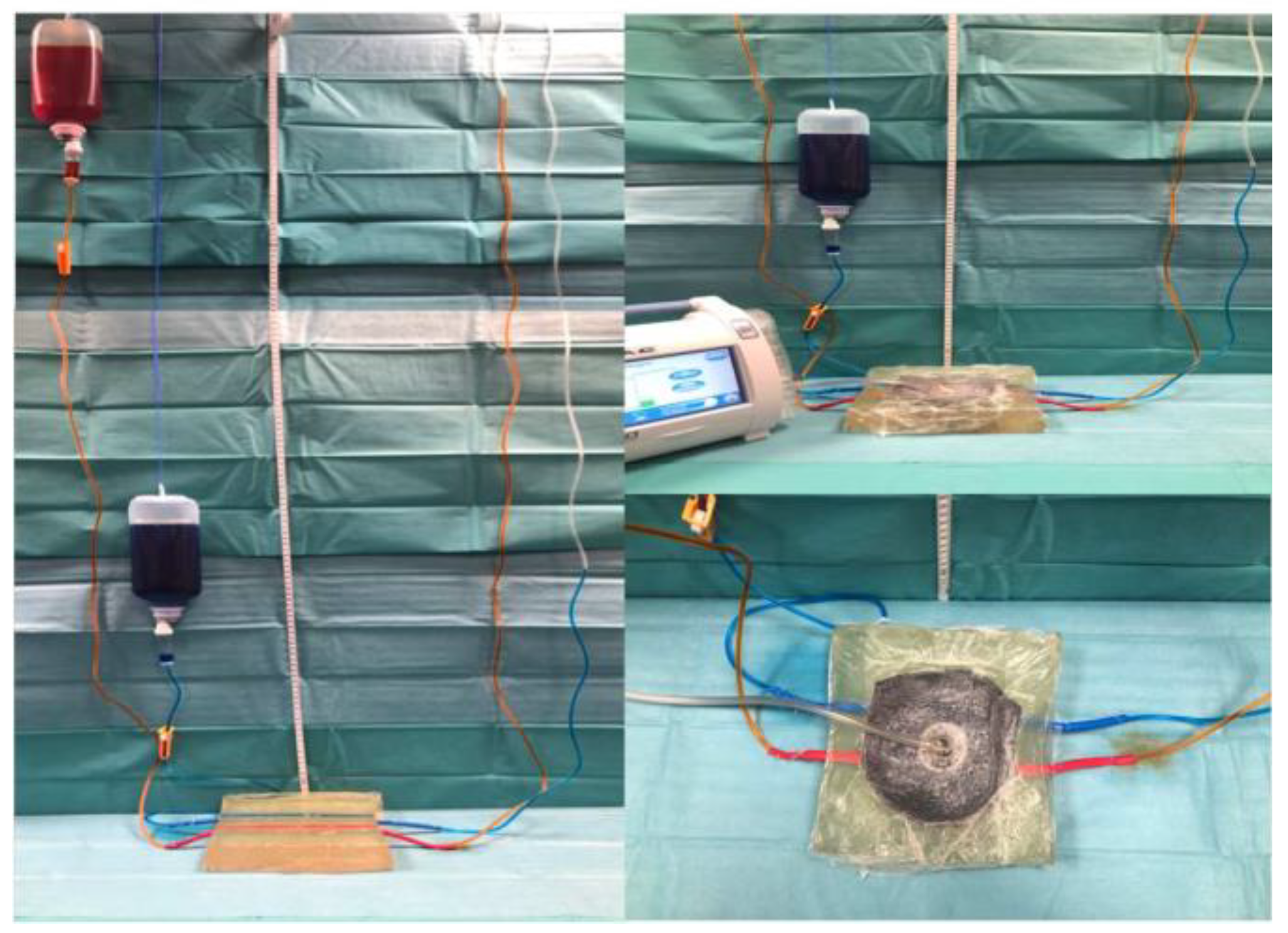
4.2. In Vitro Vessel Perfusion Model
4.3. Statistics
5. Results
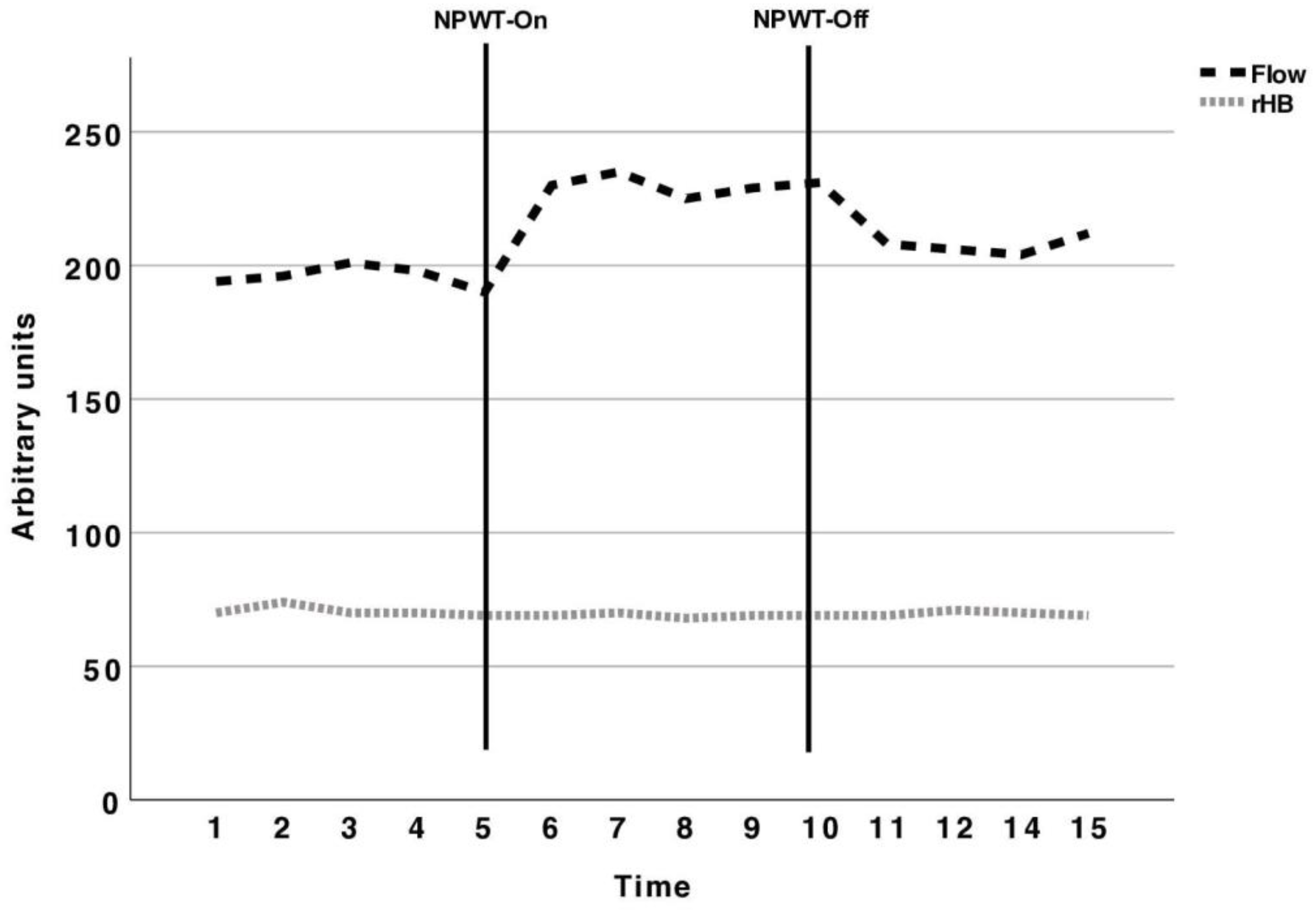
5.1. Perfusion Measurement with the O2C
5.2. Perfusion Measurement with the Masimo Rad-97®
5.3. NPWT Device in Arterial and Venous Perfusion
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biermann, N.; Geissler, E.K.; Brix, E.; Schiltz, D.; Muehle, C.; Prantl, L.; Taeger, C.D. Pressure distribution and flow characteristics during negative pressure wound therapy. J. Tissue Viability 2020, 29, 32–36. [Google Scholar] [CrossRef]
- Biermann, N.; Geissler, E.K.; Brix, E.; Schiltz, D.; Prantl, L.; Kehrer, A.; Taeger, C.D. Oxygen levels during negative pressure wound therapy. J. Tissue Viability 2019, 28, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Lobach, V.; Holton, T. Use of Closed-Incision Negative-Pressure Therapy in Aesthetic Surgery. Plast. Reconstr. Surg. 2019, 143, 11S–14S. [Google Scholar] [CrossRef]
- Gabriel, A.; Maxwell, G.P. Economic Analysis Based on the Use of Closed-Incision Negative-Pressure Therapy after Postoperative Breast Reconstruction. Plast. Reconstr. Surg. 2019, 143, 36S–40S. [Google Scholar] [CrossRef] [PubMed]
- Karlakki, S.; Brem, M.; Giannini, S.; Khanduja, V.; Stannard, J.; Martin, R. Negative pressure wound therapy for managementof the surgical incision in orthopaedic surgery: A review of evidence and mechanisms for an emerging indication. Bone Joint Res. 2013, 2, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Muller-Sloof, E.; de Laat, H.E.W.; Hummelink, S.L.M.; Peters, J.W.B.; Ulrich, D.J.O. The effect of postoperative closed incision negative pressure therapy on the incidence of donor site wound dehiscence in breast reconstruction patients: DEhiscence PREvention Study (DEPRES), pilot randomized controlled trial. J. Tissue Viability 2018, 27, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Peinemann, F. Negative Pressure Wound Therapy: Randomised Controlled Trials from 2000 to 2015. Zentralbl. Chir. 2017, 142, 267–274. [Google Scholar] [PubMed]
- Pliakos, I.; Michalopoulos, N.; Papavramidis, T.S.; Arampatzi, S.; Diza-Mataftsi, E.; Papavramidis, S. The effect of vacuum-assisted closure in bacterial clearance of the infected abdomen. Surg. Infect. 2014, 15, 18–23. [Google Scholar] [CrossRef]
- Schlosser, K.A.; Otero, J.; Lincourt, A.; Augenstein, V.A. Management of Surgical Incisions Using Incisional Negative-Pressure Therapy. Plast. Reconstr. Surg. 2019, 143, 15S–20S. [Google Scholar] [CrossRef]
- Orgill, D.P.; Manders, E.K.; Sumpio, B.E.; Lee, R.C.; Attinger, C.E.; Gurtner, G.C.; Ehrlich, H.P. The mechanisms of action of vacuum assisted closure: More to learn. Surgery 2009, 146, 40–51. [Google Scholar] [CrossRef]
- Glass, G.E.; Murphy, G.F.; Esmaeili, A.; Lai, L.M.; Nanchahal, J. Systematic review of molecular mechanism of action of negative-pressure wound therapy. Br. J. Surg. 2014, 101, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Sogorski, A.; Lehnhardt, M.; Goertz, O.; Harati, K.; Kapalschinski, N.; Hirsch, T.; Daigeler, A.; Kolbenschlag, J. Improvement of local microcirculation through intermittent Negative Pressure Wound Therapy (NPWT). J. Tissue Viability 2018, 27, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Atkins, B.Z.; Tetterton, J.K.; Petersen, R.P.; Hurley, K.; Wolfe, W.G. Laser Doppler flowmetry assessment of peristernal perfusion after cardiac surgery: Beneficial effect of negative pressure therapy. Int. Wound J. 2011, 8, 56–62. [Google Scholar] [CrossRef]
- Petzina, R.; Gustafsson, L.; Mokhtari, A.; Ingemansson, R.; Malmsjo, M. Effect of vacuum-assisted closure on blood flow in the peristernal thoracic wall after internal mammary artery harvesting. Eur. J. Cardio-Thoracic Surg. 2006, 30, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Li, Z.; Shou, K.; Jian, C.; Li, P.; Niu, Y.; Qi, B.; Yu, A. Negative pressure wound therapy: Regulating blood flow perfusion and microvessel maturation through microvascular pericytes. Int. J. Mol. Med. 2017, 40, 1415–1425. [Google Scholar] [CrossRef]
- Malmsjo, M.; Ingemansson, R.; Martin, R.; Huddleston, E. Wound edge microvascular blood flow: Effects of negative pressure wound therapy using gauze or polyurethane foam. Ann. Plast. Surg. 2009, 63, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Argenta, L.C.; Morykwas, M.J. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann. Plast. Surg. 1997, 38, 563–576; discussion 577. [Google Scholar] [CrossRef] [PubMed]
- Ichioka, S.; Watanabe, H.; Sekiya, N.; Shibata, M.; Nakatsuka, T. A technique to visualize wound bed microcirculation and the acute effect of negative pressure. Wound Repair Regen. 2008, 16, 460–465. [Google Scholar] [CrossRef]
- Timmers, M.S.; Le Cessie, S.; Banwell, P.; Jukema, G.N. The effects of varying degrees of pressure delivered by negative-pressure wound therapy on skin perfusion. Ann. Plast. Surg. 2005, 55, 665–671. [Google Scholar] [CrossRef]
- Wood, B.C.; Molnar, J.A. Subatmospheric pressure therapy: Basic science review. J. Surg. Orthop. Adv. 2011, 20, 168–175. [Google Scholar]
- Tanaka, M.; Takahashi, Y.; Hasegawa, K.; Ito, Y.; Nemoto, T.; Isogai, Z. The mechanism of persistent undermining of a sacral pressure ulcer: Experimental analyses using a deformable model and examination of skin mobility over different anatomical locations. J. Tissue Viability 2020, 29, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Borgquist, O.; Anesater, E.; Hedstrom, E.; Lee, C.K.; Ingemansson, R.; Malmsjo, M. Measurements of wound edge microvascular blood flow during negative pressure wound therapy using thermodiffusion and transcutaneous and invasive laser Doppler velocimetry. Wound Repair Regen. 2011, 19, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Borgquist, O.; Ingemansson, R.; Malmsjo, M. Wound edge microvascular blood flow during negative-pressure wound therapy: Examining the effects of pressures from −10 to −175 mmHg. Plast. Reconstr. Surg. 2010, 125, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Solomons, M.; Hudson, D.A. Negative-pressure wound therapy I: The paradox of negative-pressure wound therapy. Plast. Reconstr. Surg. 2009, 123, 589–598; discussion 599–600. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Holmes, W.J.M.; Solomons, M.; Hudson, D.A.; Kahn, D. Does a zone of increased perfusion exist around negative-pressure dressings? Plast. Reconstr. Surg. 2013, 132, 978–987. [Google Scholar] [CrossRef]
- Kairinos, N.; McKune, A.; Solomons, M.; Hudson, D.A.; Kahn, D. The flaws of laser Doppler in negative-pressure wound therapy research. Wound Repair Regen. 2014, 22, 424–429. [Google Scholar] [CrossRef]
- Muenchow, S.; Horch, R.E.; Dragu, A. Effects of topical negative pressure therapy on perfusion and microcirculation of human skin. Clin. Hemorheol. Microcirc. 2019, 72, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Voogd, A.M.; Botha, P.H.; Kotze, T.; Kahn, D.; Hudson, D.A.; Solomons, M. Negative-pressure wound therapy II: Negative-pressure wound therapy and increased perfusion. Just an illusion? Plast. Reconstr. Surg. 2009, 123, 601–612. [Google Scholar] [CrossRef]
- Kumar, S.; Samraj, K.; Nirujogi, V.; Budnik, J.; Walker, M.A. Intermittent pneumatic compression as an adjuvant therapy in venous ulcer disease. J. Tissue Viability 2002, 12, 42–50. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | NPWT-On Phase (p-Value of Comparison to Baseline) | NPWT-Off Phase (p-Value of Comparison to Baseline) | |
|---|---|---|---|
| Flow | 194 AUs | 230 AUs (0.09) | 208 AUs (0.12) |
| rHB | 70 AUs | 69 AUs/(0.77) | 69.6 AUs (0.74) |
| Baseline | NPWT-On Phase (p-Value of Comparison to Baseline) | NPWT-Off Phase (p-Value of Comparison to Baseline) | |
|---|---|---|---|
| Saturation | 92.91% | 94.11% (0.21) | 93.11% (0.68) |
| Perfusion Index | 0.17% | 0.32% (0.04) | 0.17% (0.72) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taeger, C.D.; Muehle, C.; Kruppa, P.; Prantl, L.; Biermann, N. Negative Pressure Wound Therapy—A Vacuum-Mediated Positive Pressure Wound Therapy and a Closer Look at the Role of the Laser Doppler. J. Clin. Med. 2024, 13, 2351. https://doi.org/10.3390/jcm13082351
Taeger CD, Muehle C, Kruppa P, Prantl L, Biermann N. Negative Pressure Wound Therapy—A Vacuum-Mediated Positive Pressure Wound Therapy and a Closer Look at the Role of the Laser Doppler. Journal of Clinical Medicine. 2024; 13(8):2351. https://doi.org/10.3390/jcm13082351
Chicago/Turabian StyleTaeger, Christian D., Clemens Muehle, Philipp Kruppa, Lukas Prantl, and Niklas Biermann. 2024. "Negative Pressure Wound Therapy—A Vacuum-Mediated Positive Pressure Wound Therapy and a Closer Look at the Role of the Laser Doppler" Journal of Clinical Medicine 13, no. 8: 2351. https://doi.org/10.3390/jcm13082351