

Understanding the Risk of Social Vulnerability for the Chinese Diaspora during the COVID-19 Pandemic: A Model Driving Risk Perception and Threat Appraisal of Risk Communication—A Qualitative Study
 , , and
, , and
Abstract
:1. Introduction
1.1. Context of Chinese Diaspora in the Greater Toronto Area (GTA), Ontario, Canada
1.2. Chinese Diaspora in Canada during the COVID-19 Pandemic (2020)
1.3. Risk Communication and Risk Perception
1.4. Research Gap and Study Purpose
2. Materials and Methods
2.1. Study Design and Research Question
2.2. Theoretical–Conceptual Framework
2.3. Researcher Characteristics and Reflexivity
2.4. Recruitment of Participants
2.5. Data Collection
- How is COVID-19 impacting you and your family’s everyday life?
- Where do you seek information about COVID-19?
- How do you feel about the COVID-19 information that you receive?
- What are the challenges of COVID-19 that you or your family/friends face?
2.6. Data Analysis
2.7. Trustworthiness
2.8. Ethical Aspects
3. Results
3.1. Participants’ Socio-Demographic Characteristics
3.2. Thematic Results: Summary
3.3. Social Vulnerability
‘So, we’re wearing masks, and a French lady neighbour came up to me and warned me not to wear masks without even asking me whether someone was sick. Just told me that “Oh you better not wear a mask to avoid the stigma because you’re Asian and wearing a mask.” I thanked her for the concern.’(#24)
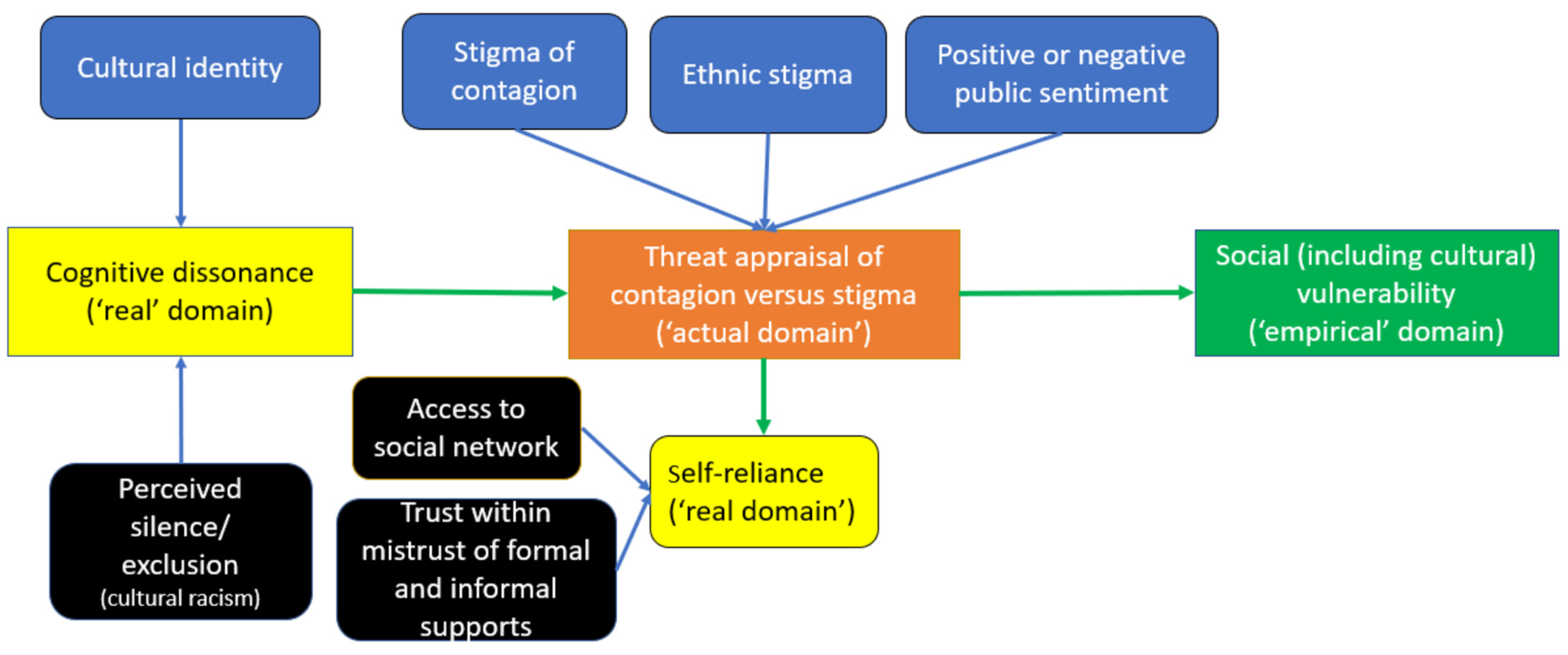
3.4. Individuals’ Threat Appraisal of Stigma Versus Contagion
- (a)
- Stigma of contagion
‘I was saying from my observation a lot of, like most Chinese people, like vast majority of Chinese people, wear masks. But like […] Canadians, a lot of them still don’t really wear masks.’(#40)
- (b)
- Ethnic stigma
‘So, if you have one member of your family that doesn’t follow the rules, he is the killer. He is the one that caused problems because he’s the weakest guy. He’s the guy who is most likely to catch the virus and, in turn, will give it to the rest of the family.’(#12)
‘I remember in 2009, there was H1N1, it originated in Mexico; they were the ones who got it first. Then it spread to many countries. I paid attention to the news at that time to see if anyone humiliated Mexican. I found out that there was none. And when it comes to COVID-19, many racists scolded, humiliated, and even hit Chinese. This is not fair for Chinese.’(#38)
- (c)
- Public sentiment
‘It really seems to me it’s about the leadership of where one is. And when I think about Trump it’s not just that he normalizes this casual racism … But I also think about Chinese people under him just getting to be more afraid even if nothing bad actually happened because they feel that target and they feel not supported in that way and I hope that people here feel a contrast, that the Chinese community feels differently.’(#25)
- (d)
- Mechanism of self-reliance to recover from adversity
‘They’re [parents] not able to go out and they hear the news, and unfortunately, most of the time, the news, it’s not too positive. They don’t have a lot of friends, so they do feel anxious and nervous because they only hear the negative news, and they don’t have a lot of friends among their network to alleviate their worry.’(#34)
‘Like an old person says, “hey, I need a grocery run” and then someone will respond. And then once it’s resolved, the thread is closed.’(#14)
‘Because I came from Hong Kong, I experienced SARS. When it seriously contradicts my opinions, I tend not to believe it, or I would look at and check with the media that I can trust.’(#66)
3.5. Risk Perception: Driving Mechanism of Cognitive Dissonance
‘I’m quite blessed, right. I haven’t been discriminated against, even before…but I would not disregard it as unimportant. I think those who treat people badly are just ignorant. To me, COVID has no boundary. No race. Nothing, right? So, everybody can catch it.’(#35)
- (a)
- Cultural identity
‘We have this debate, and I am telling him that you shouldn’t buy masks for everyone because of public relations. I don’t want people to see Chinatown purchase a bunch of masks and give it to frontline people, because I know we’ll be attacked.’(#7)
- (b)
- Perceived public silence and/or exclusion in groups (cultural racism)
‘It’s a feeling of not having much understanding and support around you, it’s even sadder. Recently, a white Canadian classmate told me… “Whatever you said at that time is now happening here.” She is also sad, and she is unsure why the so-called mainstream, so-called official, so-called government here in Canada had not been able to hear the voices of the Chinese and the emotions of the people like me.’(#80)
‘People like my parents who do not speak much English only receive information from Chinese sources so they do not know much from the Canadian side, and maybe they are just hearing about the numbers and scared but they are not hearing all the other information that they do not understand in English.’(#42)
‘In the beginning, I was very serious… But after a while, I felt like I couldn’t bear it anymore. It was very hard. So, I read something funny. I watched some Hong Kong comedy from before, and later, I also cooked. I cooked and talked about things related to cooking and other more positive things. Tried to feel everything is okay, and I also listened to the radio.’(#41)
4. Discussion
4.1. Implications for Health Policy
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization [WHO]. Attacks on Health Care in the Context of COVID-19. 2020. Available online: https://www.who.int/news-room/feature-stories/detail/attacks-on-health-care-in-the-context-of-covid-19 (accessed on 3 November 2022).
- Nezafat Maldonado, B.M.; Collins, J.; Blundell, H.J.; Singh, L. Engaging the vulnerable: A rapid review of public health communication aimed at migrants during the COVID-19 pandemic in Europe. J. Migr. Health 2020, 1, 100004. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Adlhoch, C.; Baka, A.; Broberg, E.; Cenciarelli, O.; De Angelis, S.; Einoder-Moreno, M.; Dalmau, I.J.Q.; Kinross, P.; Kinsman, J.; et al. COVID-19 research priorities for nonpharmaceutical public health and social measures. Epidemiol. Infect. 2021, 149, e87. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, M.M.; Arnout, B.A.; Fadhel, F.H.; Sufyan, N.S.S. Risk perceptions of COVID-19 and its impact on precautionary behavior: A qualitative study. Patient Educ. Couns. 2021, 104, 1860–1867. [Google Scholar] [CrossRef]
- Kline, N.S. Rethinking COVID-19 vulnerability: A call for LGBTQ+ Im/migrant health equity in the United States during and after a pandemic. Health Equity 2020, 4, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Poston, D.L.; Wong, J.H. The Chinese diaspora: The current distribution of the overseas Chinese population. Chin. J. Sociol. 2016, 2, 348–373. [Google Scholar] [CrossRef]
- Gao, Z. Unsettled belongings: Chinese immigrants’ mental health vulnerability as a symptom of international politics in the COVID-19 pandemic. J. Humanist. Psychol. 2021, 61, 198–218. [Google Scholar] [CrossRef]
- Leung, V.W.Y.; Tan, W.; Chuang, D.-M.; Tsang, K.T.; Lai, D.W.L. A Multidimensional approach to explore the experiences with ethnic matching amongst Chinese social service practitioners in the Greater Toronto Area. Br. J. Soc. Work. 2022, 52, 1592–1611. [Google Scholar] [CrossRef]
- Stats Canada. Census Profile, 2021 Census Population. Toronto, Ontario 2021. Census Metropolitan Area. Available online: https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/details/page.cfm?Lang=E&GENDERlist=1,2,3&STATISTIClist=1,4&HEADERlist=0&DGUIDlist=2021S0503535&SearchText=Toronto (accessed on 29 June 2023).
- Toronto Public Health. Toronto COVID-19 Monitoring Dashboard by Surveillance & Epidemiology; Toronto Public Health: Toronto, ON, Canada, 2021. Available online: https://public.tableau.com/app/profile/tphseu/viz/TorontoCOVID-19MonitoringDashboard/MainReportCard (accessed on 21 June 2023).
- Stats Canada. Immigration and Ethnocultural Diversity; Stats Canada: Ottawa, ON, Canada, 2022. Available online: https://www150.statcan.gc.ca/n1/dai-quo/ssi/homepage/rel-com/theme43-eng.htm (accessed on 3 November 2022).
- Yu, L.; Lecompte, M.; Zhang, W.; Wang, P.; Yang, L. Sociodemographic and COVID-related predictors for mental health condition of Mainland Chinese in Canada amidst the pandemic. Int. J. Environ. Res. Public Health 2022, 19, 171. [Google Scholar] [CrossRef] [PubMed]
- Dean, L.T.; Thorpe, R.J. What structural racism is (or is not) and how to measure it: Clarity for public health and medical researchers. Am. J. Epidemiol. 2022, 191, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- Stats Canada. Perceptions of Personal Safety among Population Groups Designated as Visible Minorities in Canada during the COVID-19 Pandemic; Stats Canada: Ottawa, ON, Canada, 2020. Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00046-eng.htm (accessed on 5 July 2022).
- Berg, S.H.; O’Hara, J.K.; Shortt, M.T.; Thune, H.; Brønnick, K.K.; Lungu, D.A.; Røislien, J.; Wiig, S. Health authorities’ health risk communication with the public during pandemics: A rapid scoping review. BMC Public Health 2021, 21, 1410. [Google Scholar] [CrossRef] [PubMed]
- Herfurth, H. What Exactly Does It Mean to ‘Flatten the Curve’? UAB Expert Defines Coronavirus Terminology for Everyday Life. 28 April 2020. Available online: https://www.uab.edu/news/youcanuse/item/11268-what-exactly-does-it-mean-to-flatten-the-curve-uab-expert-defines-coronavirus-terminology-for-everyday-life (accessed on 15 March 2022).
- Sutton, J.; Rivera, Y.; Sell, T.K.; Moran, M.B.; Bennett Gayle, D.; Schoch-Spana, M.; Stern, E.K.; Turetsky, D. Longitudinal risk communication: A research agenda for communicating in a pandemic. Health Secur. 2021, 19, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Gesser-Edelsburg, A. Analysis of the government of Israel’s COVID-19 health and risk communication efforts: Between a political-constitutional crisis and a health crisis. In Communicating COVID-19: Interdisciplinary Perspectives; Palgrave Macmillan: Cham, Switzerland, 2021; pp. 203–225. [Google Scholar] [CrossRef]
- Yaussy, S. Intersectionality and the interpretation of past pandemics. Bioarchaeol. Int. 2022, 6, 58–76. [Google Scholar] [CrossRef]
- Maloney, E.K.; Lapinski, M.K.; Witte, K. Fear Appeals and Persuasion: A Review and Update of the Extended Parallel Process Model. Soc. Personal. Psychol. Compass 2011, 5, 206–219. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. COVID-19 and the Social Determinants of Health and Health Equity: Evidence Brief; World Health Organization: Geneva, Switzerland, 2021; Licence: CC BY-NC-SA 3.0 IGO; Available online: https://www.who.int/publications/i/item/9789240038387 (accessed on 3 November 2022).
- Wittenberg, E.; Goldsmith, J.V.; Chen, C.; Prince-Paul, M.; Johnson, R.R. Opportunities to improve COVID-19 provider communication resources: A systematic review. Patient Educ. Couns. 2021, 104, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.; Martinho, A.L. Social vulnerability as the intersection of tangible and intangible variables: A proposal from an inductive approach. Rev. Nac. Adm. 2021, 12, e3773. [Google Scholar]
- Mah, J.; Rockwood, K.; Stevens, S.; Keefe, J.; Andrew, M. Do interventions reducing social vulnerability improve health in community dwelling older adults? A systematic review. Clin. Interv. Aging 2022, 17, 447–465. [Google Scholar] [CrossRef] [PubMed]
- Ho, E.L.-E.; Maddrell, A. Intolerable intersectional burdens: A COVID-19 research agenda for social and cultural geographies. Soc. Cult. Geogr. 2021, 22, 1–10. [Google Scholar] [CrossRef]
- Adekunle, T.B.; Mohammed, W.F. Communication in context: How culture, structure, and agency shape health and risk communication about COVID-19 in Ghana. World Med. Health Policy 2022, 14, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Mamuji, A.; Lee, C.; Rozdilsky, J.; D’Souza, J.; Chu, T. Anti-Chinese stigma in the Greater Toronto Area during COVID-19: Aiming the spotlight towards community capacity. Soc. Sci. Humanit. Open 2021, 4, 100232. [Google Scholar] [CrossRef] [PubMed]
- Elder-Vass, D. Normative institutions. In Critical Realism and the Causal Power of Social Structures; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Wiltshire, G.; Ronkainen, N. A realist approach to thematic analysis: Making sense of qualitative data through experiential, inferential and dispositional themes. J. Crit. Realism 2021, 20, 159–180. [Google Scholar] [CrossRef]
- De Souza, D.E. Culture, context and society—The underexplored potential of critical realism as a philosophical framework for theory and practice. Asian J. Soc. Psychol. 2014, 17, 141–151. [Google Scholar] [CrossRef]
- Harwood, L.; Clark, A.M. Understanding health decisions using critical realism: Home-dialysis decision-making during chronic kidney disease. Nurs. Inq. 2012, 19, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Bower, R.A.; Coad, J.E.; Manning, J.C.; Pengelly, T.A. A qualitative, exploratory study of nurses’ decision-making when interrupted during medication administration within the Paediatric Intensive Care Unit. Intensive Crit. Care Nurs. 2018, 44, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo. 2020. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 3 May 2020).
- Fryer, T. A critical realist approach to thematic analysis: Producing causal explanations. J. Crit. Realism 2022, 21, 365–384. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Cooper, J. Cognitive dissonance: Where we’ve been and where we’re going. Int. Rev. Soc. Psychol. 2019, 32, 7. [Google Scholar] [CrossRef]
- Gehlbach, D.; Vázquez, E.; Ortiz, G.; Li, E.; Sánchez, C.B.; Rodríguez, S.; Pozar, M.; Cheney, A.M. Perceptions of the Coronavirus and COVID-19 testing and vaccination in Latinx and Indigenous Mexican immigrant communities in the Eastern Coachella Valley. BMC Public Health 2022, 22, 1019. [Google Scholar] [CrossRef] [PubMed]
- Nöstlinger, C.; Van Landeghem, E.; Vanhamel, J.; Rotsaert, A.; Manirankunda, L.; Ddungu, C.; Reyniers, T.; Katsuva, D.; Vercruyssen, J.; Dielen, S.; et al. COVID-19 as a social disease: Qualitative analysis of COVID-19 prevention needs, impact of control measures and community responses among racialized/ethnic minorities in Antwerp, Belgium. Int. J. Equity Health 2022, 21, 67. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 174. [Google Scholar] [CrossRef] [PubMed]
- Vargas, N.; Mora, G.C.; Gleeson, S. Race and ideology in a pandemic: White privilege and patterns of risk perception during COVID-19. Soc. Probl. 2021, 70, 219–237. [Google Scholar] [CrossRef]
- Scambler, G. Critical realism, sociology and health inequalities: Social class as a generative mechanism and its media of enactment. Alethia 2001, 4, 35–42. [Google Scholar] [CrossRef]
- Archer, M. Chapter 20. Addressing the cultural system. In Critical Realism, Essential Readings; Routledge Publishers: London, UK, 1998; pp. 503–543. [Google Scholar]
- Vaidis, D.C.; Bran, A. Respectable challenges to respectable theory: Cognitive dissonance theory requires conceptualization clarification and operational tools. Front. Psychol. 2019, 10, 1189. [Google Scholar] [CrossRef] [PubMed]
- Reed, H. When the right thing to do is also the wrong thing: Moral sensemaking of responsible business behavior during the COVID-19 crisis. Bus. Soc. 2022, 63, 1030–1062. [Google Scholar] [CrossRef]
- Pearce, L.; Cooper, J. Fostering COVID-19 safe behaviors using cognitive dissonance. Basic Appl. Soc. Psychol. 2021, 43, 267–282. [Google Scholar] [CrossRef]
- Chakraborty, T.; Kumar, A.; Upadhyay, P.; Dwivedi, Y.K. Link between social distancing, cognitive dissonance, and social networking site usage intensity: A country-level study during the COVID-19 outbreak. Internet Res. 2021, 31, 419–456. [Google Scholar] [CrossRef]


{kind=link}
| Frequency (n) | Percentage % (Rounded Up) | |
|---|---|---|
| Age | ||
| ≤18 years | 7 | 19 |
| 25–64 years old | 23 | 64 |
| 65–74 years old | 6 | 17 |
| Self-Identified Gender | ||
| Female | 23 | 64 |
| Male | 13 | 36 |
| Living in the Greater Toronto Area | ||
| 1–5 years | 9 | 25 |
| 6+ years | 27 | 75 |
| Self-Identified Ethnic Origin | ||
| Hong Kong | 15 | 42 |
| Mainland China | 11 | 31 |
| Taiwan | 3 | 8 |
| Other Chinese | 2 | 5 |
| Did not specify | 5 | 14 |
| Employment Status | ||
| Employed | 19 | 53 |
| Unemployed | 6 | 17 |
| Student | 5 | 14 |
| Retired | 6 | 17 |
| Self-Reported Stigma/Racism/Microaggression during COVID-19 | ||
| Yes, direct | 19 | 53 |
| Yes, indirect | 6 | 17 |
| Denies | 11 | 30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, D.Y.L.; Hwu, H.; Khan, S.; Mamuji, A.; Rozdilsky, J.; Chu, T.; Lee, C. Understanding the Risk of Social Vulnerability for the Chinese Diaspora during the COVID-19 Pandemic: A Model Driving Risk Perception and Threat Appraisal of Risk Communication—A Qualitative Study. Int. J. Environ. Res. Public Health 2024, 21, 512. https://doi.org/10.3390/ijerph21040512
Leung DYL, Hwu H, Khan S, Mamuji A, Rozdilsky J, Chu T, Lee C. Understanding the Risk of Social Vulnerability for the Chinese Diaspora during the COVID-19 Pandemic: A Model Driving Risk Perception and Threat Appraisal of Risk Communication—A Qualitative Study. International Journal of Environmental Research and Public Health. 2024; 21(4):512. https://doi.org/10.3390/ijerph21040512
Chicago/Turabian StyleLeung, Doris Yuet Lan, Hilary Hwu, Shoilee Khan, Aaida Mamuji, Jack Rozdilsky, Terri Chu, and Charlotte Lee. 2024. "Understanding the Risk of Social Vulnerability for the Chinese Diaspora during the COVID-19 Pandemic: A Model Driving Risk Perception and Threat Appraisal of Risk Communication—A Qualitative Study" International Journal of Environmental Research and Public Health 21, no. 4: 512. https://doi.org/10.3390/ijerph21040512