Calcified Tissue International ( IF 4.2 ) Pub Date : 2024-01-09 , DOI: 10.1007/s00223-023-01169-x Arthur Michon-Colin , Elise Bouderlique , Dominique Prié , Gérard Maruani , Jérôme Nevoux , Karine Briot , Marie Courbebaisse
|
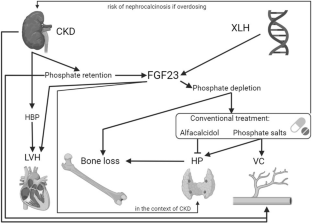
X-linked hypophosphatemic rickets (XLH) is a genetic cause of renal hypophosphatemia due to inactivation of the PHEX gene, with an inappropriate concentration of fibroblast growth factor 23 (FGF23). Burosumab, an anti-FGF23 monoclonal antibody, is a validated treatment for XLH, but its use in patients with chronic kidney disease (CKD) has not been validated. A 61-year-old man with XLH developed CKD during follow-up. Conventional treatment (phosphate salts and active vitamin D analogs) was poorly tolerated. Treatment with burosumab was decided at a multi-professional meeting. Before burosumab initiation, his measured glomerular filtration rate was 44 mL/min/1.73 m2 defining CKD stage 3b and intact FGF23 concentration was very high (4496.0 ng/mL, N: 22.7–93.1) due to both XLH and CKD. Severe hypophosphatemia was observed after the two first injections of burosumab at usual doses (1 mg/kg monthly) and concomitant discontinuation of the conventional treatment. After increasing the dose and reducing the interval between doses (1.3 mg/kg every three weeks) from the third injection, serum phosphate concentration normalized and remained around the lower limit of the normal range. A local cutaneous reaction was observed just after the second injection, but did not recur. We report for the first time the efficacy and good short-term tolerance of burosumab in a patient with XLH and CKD, subject to a higher dosage aimed at achieving a phosphatemia at the lower limit of the normal range.
中文翻译:
Burosumab 成功治疗 X 连锁低磷血症和慢性肾病 3b 期成年患者
X 连锁低磷血症性佝偻病 (XLH) 是由于 PHEX 基因失活以及成纤维细胞生长因子 23 (FGF23) 浓度不适当而导致肾性低磷血症的遗传原因。Burosumab 是一种抗 FGF23 单克隆抗体,是一种经过验证的 XLH 治疗方法,但其在慢性肾病 (CKD) 患者中的使用尚未经过验证。一名患有 XLH 的 61 岁男性在随访期间发展为 CKD。传统治疗(磷酸盐和活性维生素 D 类似物)的耐受性较差。burosumab 治疗是在多专业会议上决定的。在开始使用 burosumab 之前,测量到的肾小球滤过率为 44 mL/min/1.73 m 2,定义为 CKD 3b 期,并且由于 XLH 和 CKD,完整 FGF23 浓度非常高(4496.0 ng/mL,N:22.7-93.1)。首次两次注射常规剂量(每月 1 mg/kg)的 burosumab 并同时停止常规治疗后,观察到严重的低磷血症。从第三次注射开始增加剂量并缩短剂量间隔(每三周1.3 mg/kg)后,血清磷酸盐浓度恢复正常并保持在正常范围下限附近。第二次注射后即观察到局部皮肤反应,但未复发。我们首次报告了 burosumab 对 XLH 和 CKD 患者的疗效和良好的短期耐受性,接受较高剂量,旨在将磷血症控制在正常范围的下限。


























 京公网安备 11010802027423号
京公网安备 11010802027423号